
Case contribution: Dr Radhiana Hassan
Clinical:
- A 12 years old male, no known medical illness
- Initially presented with RIF pain for one day, dull in nature non-radiating. Also had loose stool. No fever, no UTI symptoms.
- Treated as AGE and discharged home.
- Subsequently had right scrotal pain radiating to inguinal region, pulling and twisting in nature, aggravated by movement and touch
- Pain is partially relieved with rest and painkillers. No fever, no UTI symptoms, no history of trauma
- Clinical examination shows normal general condition. Abdomen was not distended, soft and non-tender. Right and left inguinal non-tender, no lymph node palpable. Right scrotum is larger than left, tender on palpation, cremastric reflex absent on the right side, trans illumination test positive
- Left scrotum and testis are normal.

Abdominal radiograph:
- No dilated bowel loops
- No obvious soft tissue mass
- No abnormal calcification seen
- Bones and soft tissues are unremarkable
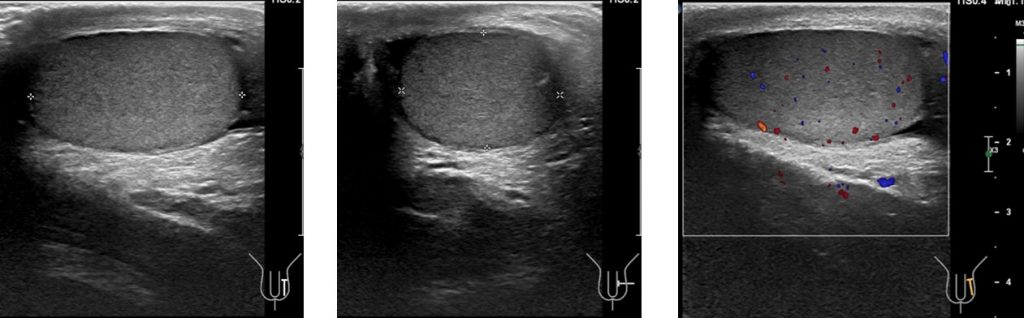
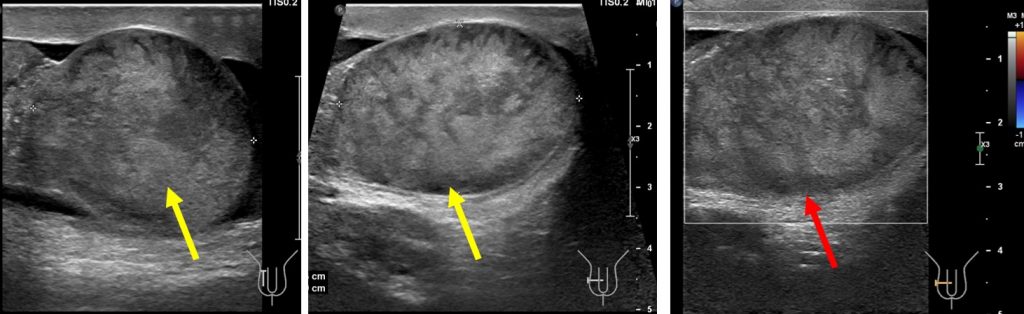
Ultrasound findings:
- The right testis appears enlarged and heterogenous in echogenicity (yellow arrows).
- The right scrotal wall is thickened.
- Right epididymis is diffusely enlarged with concentric layering.
- No vascularity is detected on Doppler assessment for the right testis and epididymis (red arrow).
- There is minimal fluid within the right scrotal sac.
- Left testis is normal.
Progress of patient:
- Urgent scrotal exploration done
- Intraoperative findings: Non-viable right testis secondary to intratunical torsion despite resuscitation, twisted x2, hemorrhagic fluids about 20cc from right scrotum, sent for HPE
- Left testis normal, 3-point orchidopexy done, straw coloured fluid about 5cc upon entering left scrotum
- Right orchidectomy and left orchidopexy performed
Diagnosis: Testicular torsion
Discussion:
- Testicular torsion is defined as the rotation of the testis along the longitudinal axis of the spermatic cord. The twisting of spermatic cord eventually leads to venous obstruction, followed by obstruction of arterial inflow and testicular ischaemia.
- It has two incidence peaks; the neonatal period and puberty, 65% occurs between 12-18 years.
- In puberty, torsion occurs within the tunica vaginalis due to a ‘bell clapper’ deformity (intravaginal torsion)
- Testicular viability depends on the duration of torsion and number of twists of spermatic cord. In low degree of torsion, testes can remain viable for more than 24 hours. In higher degree torsion infarction can occur as soon as 4 hours post-onset of scrotal pain.
- Gray scale and doppler ultrasound is the imaging modality of choice. Findings can varies and features are non-specific
- Swollen and hypoechoic (4-6 hours) or a heterogenous (24 hours-infarcted) testis
- Thickened epididymis and spermatic cord
- Reactive hydrocele
- The whirlpool sign = twisting of the spermatic cord at the external inguinal ring
- Doppler-absence or reduction of blood flow
- If blood flow is present (partial torsion), spectral waveform demonstrate high-resistance flow (RI>0.75) and decreased diastolic flow or diastolic flow reversal.
- Differential diagnoses: epididymo-orchitis, testicular tumour or testicular trauma
Recent Comments