
Case contribution: Dr Radhiana Binti Hassan
Clinical:
- A 78 years old lady with underlying HPT, DM, CKD, dyslipidaemia and IHD
- Presented with left breast swelling for one year
- No pain, no fever, no nipple discharge, no constitutional symptoms
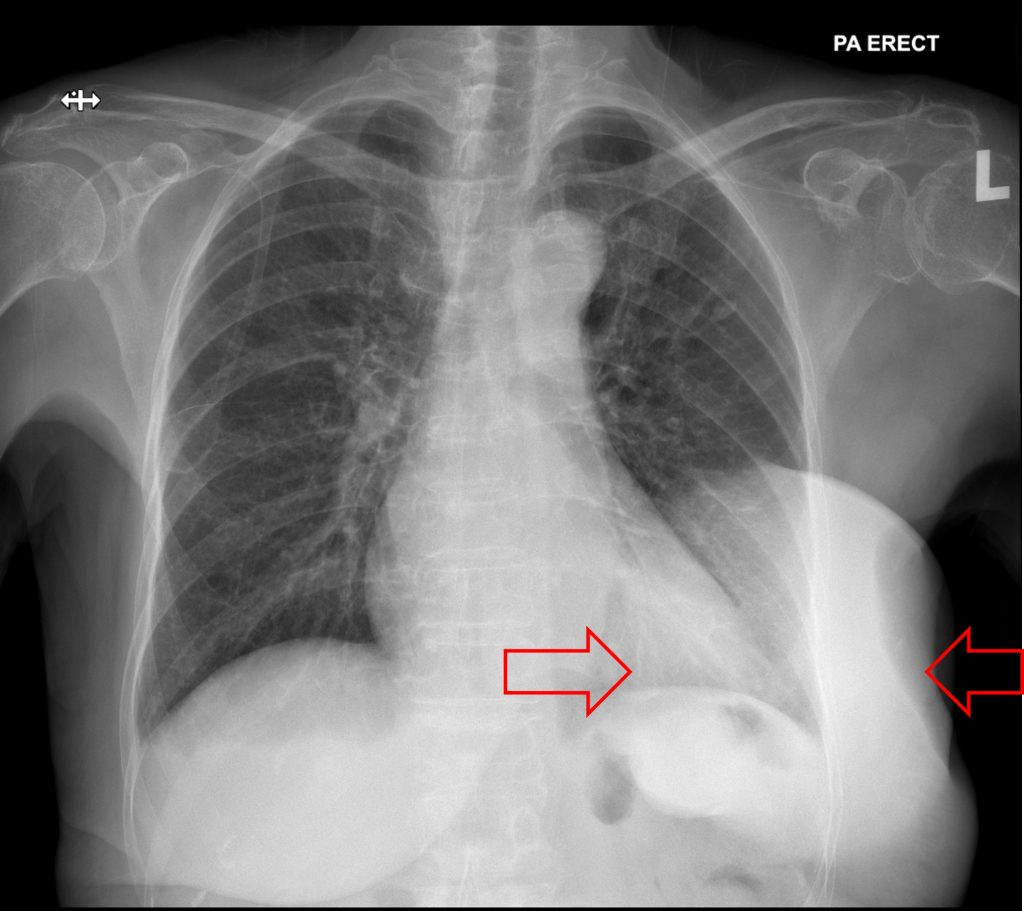
Chest radiograph:
- A huge rounded well-defined opacity overlying the lower left thoracic region
- There is no obliteration of cardiac border or outline of hemidiaphragm
- No calcification within the lesion. No fluid levels within.
- Left costophrenic angle is sharp. No bone change.
- Soft tissue at left axillary region is prominent compared to the right side.
- Visualized lungs are clear. No hilar mass.
- No cardiomegaly. Bones are normal.
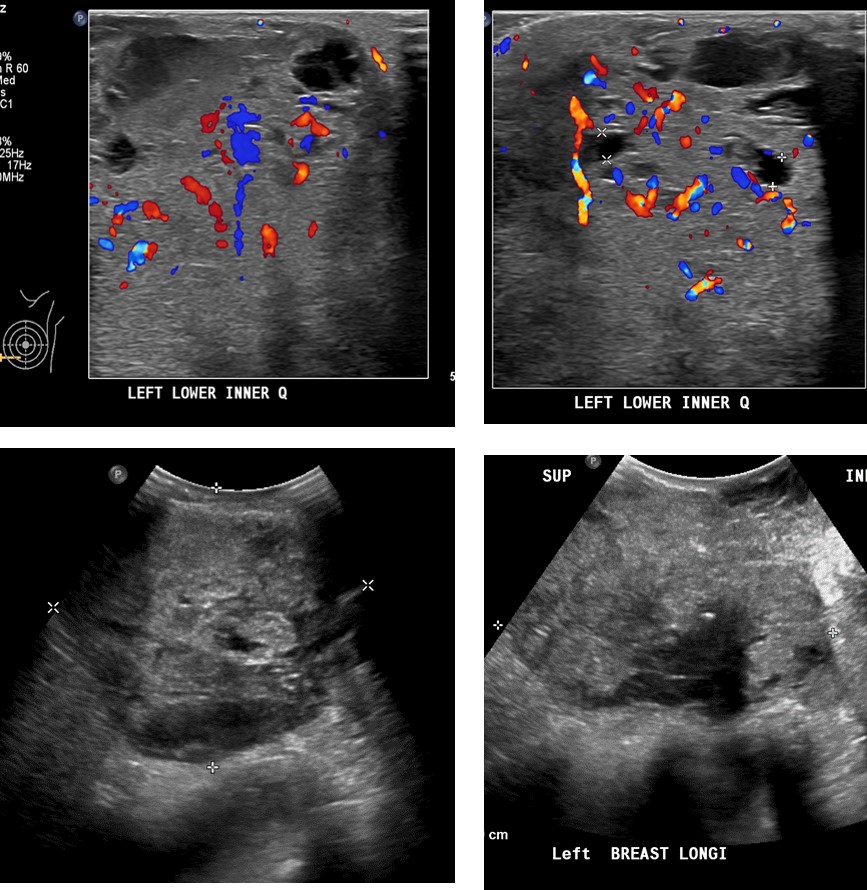
Ultrasound findings:
- A large predominantly solid heterogeneous hyperechoic mass is occupying the entire left breast measuring approximately 9.0 x 10.1 x 11.0 cm (AP x W x CC).
- Multiple intralesional vascularity within this solid mass.
- At the lower inner quadrant of this mass, there is an exophytic multiseptated cystic mass measuring 2.0 x 4.0 x 3.6 cm. Mobile internal echogenic debris is seen within.
- The underlying pectoral muscle is not well visualised.
- Few hypoechoic tubular structures measuring up to 0.4 cm in diameter are seen scattered within the breast with no internal vascularity, likely dilated ducts.
- There are several enlarged well defined heterogeneous hypoechoic axillary lymph nodes with loss of fatty hilum, largest measuring 1.6 x 3.5 x 3.7 cm.
- The overlying skin is thickened.
Core biopsy:
- Features are suggestive of malignant mesenchymal neoplasm.
- Differential diagnoses: malignant phylloides tumour, sarcoma of the breast and metaplastic carcinoma.
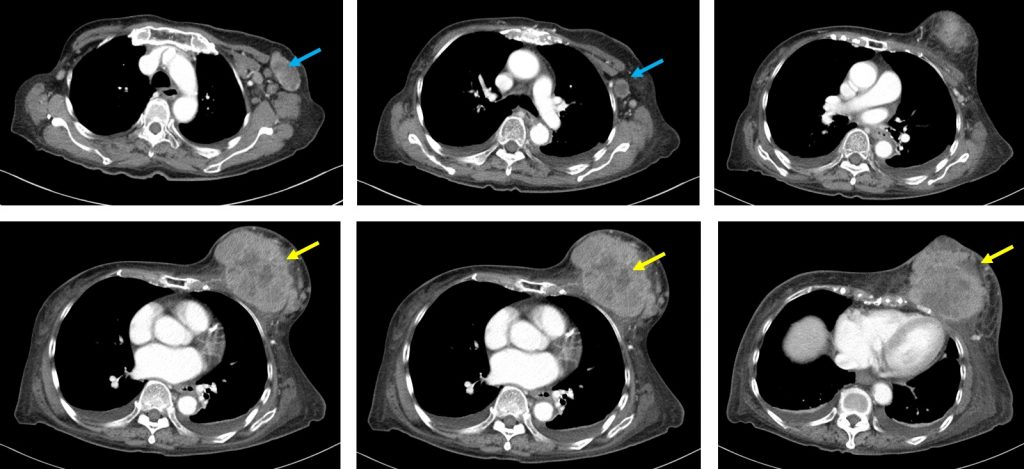
CT scan findings:
- A huge lobulated heterogenous enhanced mass (yellow arrows) is seen occupying the left breast. It measures about 9.4 x 9.2 x 12.0 cm (AP x W x CC).
- A few hypodensities are seen within the mass likely represent necrotic components.
- No intralesional calcification.
- There is poor plane of demarcation of the mass with the underlying pectoralis muscles. This muscle is thickened and stranding suggestive of involvement.
- Superficially, it involved the overlying skin and nipple causing thickening of the overlying skin and nipple retraction. It is associated with surrounding subcutaneous tissue oedema.
- No local bone rib destruction seen.
- Multiple enlarged left axillary lymph nodes (blue arrows) are seen with the largest measuring about 4.7 x 2.2 cm (AP x W). Hypodensity seen within some the nodes in keeping with necrotic area.
- No focal enhancing right breast lesion.
HPE from left mastectomy specimen:
- Metaplastic carcinoma with heterologous mesenchymal differentiation.
- There are two components seen:
- invasive carcinoma (20%)
- mesenchymal differentiation (80%)-chondroid and osseous differentiation with chondroid and osseous matrix
- No DCIS. No LCIS.
- Presence of lympovascular invasion.
- No microcalcification seen
- All 12 left axillary nodes are positive of tumour infiltration
Diagnosis: Metaplastic carcinoma with heterologous mesenchymal differentiation.
Discussion:
- Most of the breast tumours arise from glandular epithelium. However, in some cases, glandular epithelium differentiates into non-glandular mesenchymal tissue, a process called metaplasia. Metaplastic changes include squamous cell, spindle cell and heterologous mesenchymal growth, occur in fewer than 5% of breast carcinomas.
- Metaplastic breast carcinomas are regarded as ductal carcinomas that undergo metaplasia into nonglandular growth pattern. These rare tumours show pathologic features of both carcinoma and sarcoma.
- Metaplastic carcinoma with a sarcomatous component is a different entity from primary breast sarcoma.
- It is usually seen in women who are more than 50 years old.
- The mammographic appearance of metaplastic breast carcinoma has been described in case reports or in small series as mass lesion which can be circumscribed, irregular, or spiculated margins. It is usually noncalcified.
- A few case reports noted presence of microcalcifications, or lesion with densely calcified center and an osteoid matrix. A case report also noted one patient with clustered microcalcifications without an associated mass.
- One ultrasound, masses showed complex internal echogenicity with solid and cystic components, which was consistent with necrosis and cystic degeneration at pathologic examination. Thus, although a rare tumor, it should be considered in the differential diagnosis of breast masses with solid and cystic components.
- The distinction between metaplastic breast cancer and sarcoma is clinically important because the surgical treatment, chemotherapy regimens, and metastatic pathways are different.
- Typically, axillary lymph node involvement is rare in breast sarcoma even when the disease is diffusely disseminated, whereas lymph node metastases are reported in 25-30% of cases with metaplastic carcinomas.
- Although no series has been sufficiently large to determine overall prognosis, survival most likely depends on tumor size, histologic type, grade, lymph node status, and perhaps most directly on the type and grade of the mesenchymal component.
- The overall 5-year survival rate is approximately 40%.
Recent Comments