
Case contribution: Dr Radhiana Hassan
Clinical:
- A 56 years old man
- No known medical problem
- Presented with behavioural change
- Clinical examination is unremarkable
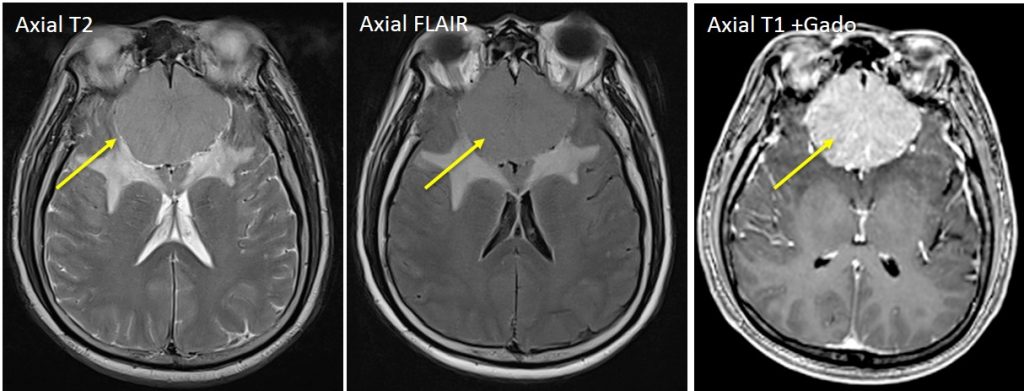
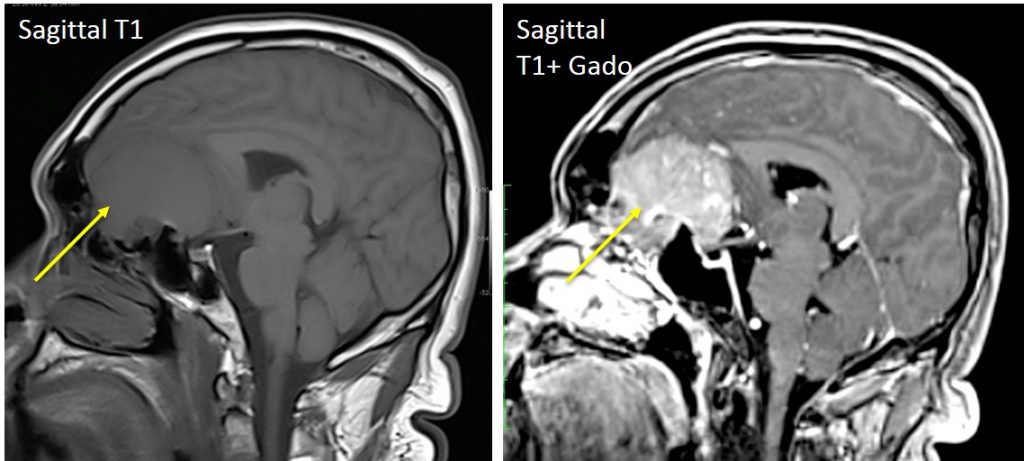
MRI findings:
- A large extra-axial mass at olfactory groove of anterior cranial fossa
- It is isointense on T1, hyperintense on T2 and vividly enhancing post contrast
- The mass exert mass effect causing posterior displacement of the frontal lobe and corpus callosum
- Vasogenic oedema of adjacent brain parenchyma
- No hydrocephalus
Histopathological findings:
- Macroscopic: multiple fragments tumoral tissue and whitish tissue labelled as falx
- Microscopic: sections of tumour tissue composed predominantly spindle-shaped cells forming parallel and interlacing bundles with occasional areas displaying sheets and lobules of whorl formation. The tumour cells have uniform nuclei with fine chromatin. No psammoma bodies seen. No areas of necrosis. No increase mitotic figure are seen. Immunohistochemical studies show the tumour cells positive for EMA (epithelial membrane antigen) and S-100. Negatives for GFAP (glial fibrillary acidic protein) and CK (cytokeratin). Ki67 proliferative index is >2%. No tumour infiltration to falx.
- Diagnosis: Fibrous meningioma-WHO Grade 1
Final diagnosis: Olfactory groove meningioma
Discussion:
- Olfactory groove meningiomas are relatively common intracranial lesions, representing approximately 4.5 – 18% percent of intracranial meningiomas
- These tumors arise from the floor of the anterior cranial fossa over the cribriform plate of the ethmoid bone.
- Due to their slow rate of growth, and their site and location in vicinity of the frontal lobes, these tumors achieve a significantly large size at the time of diagnosis and have relatively innocuous presenting clinical signs.
- A large tumor size, a firm and vascular nature, extension on both sides of the midline and a wide basal attachment are the general characteristics.
- There is female preponderance.
- Most tumors were encountered in patients in the third to fourth decade of life.
- The presence of calcification on preoperative imaging was indicative of the firm nature of the tumor.
- The presence of enostosis and hyperostosis was seen in the firmer varieties of tumor.
- The presence and extent of cerebral edema on imaging was indicative of the rate of growth of the tumor, reaction from the brain and the intimacy of brain-tumor interface.
Progress of patient:
- craniotomy and tumour excision done
- complicated by CSF leak from nose
- subsequent MRI assessment showed defect at cribriform plate
- laparoscopic repair of CSF-rhinorrhoea done
- Follow up after 2 years showed no recurrence of lesion
Recent Comments