
Case contribution: Dr Radhiana Hassan
Clinical:
- A 65 years old lady with no underlying medical illness
- She presented with progressive left upper and lower limbs weakness for 2 months.
- No history of trauma. No fever. No headache.
- Clinical examination shows power or left upper limb and lower limb 3/5.
- Other examinations are unremarkable.
- CT brain shows cystic lesion in the right parietal lobe.
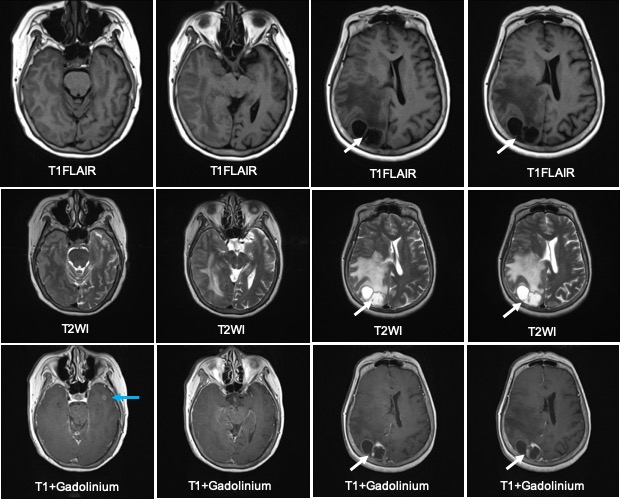
MRI findings:
- There are cystic lesions with peripheral ring enhancement seen at the right parietal lobe measuring 1.9(AP)x3.8(w)x3.1(CC)
- It is associated with vasogenic oedema and effacement of ipsilateral cortical sulcation.
- It causes mass effect and compression to the posterior horn of the right lateral ventricle and causes minimal midline shift to the left.
- Multiple smaller ring enhancing lesions are also seen in the grey white matter junction of left temporal horn (blue arrow) and vermis.
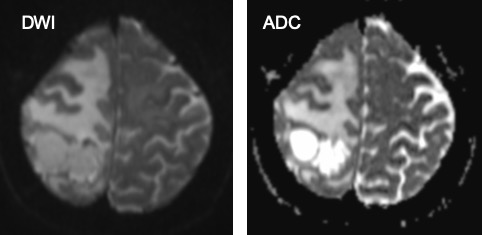
- These lesions do not demonstrate diffusion restriction.
- No obvious calcificaiton of haemorrhagic components seen. No hydrocephalus.
- No abnormal meningeal enhancement post contrast.
Progress of patient:
- TB work out was negative
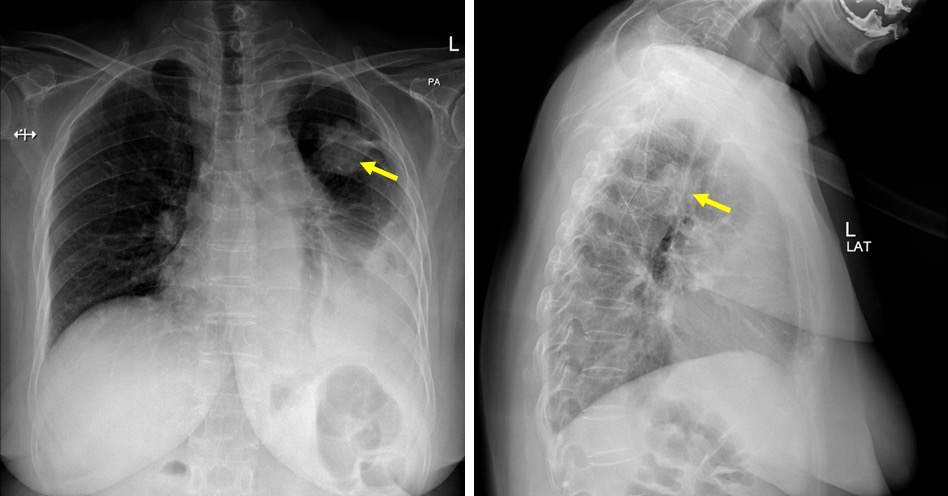
- CXR and CT thorax show suspicious mass lesion in the left lung
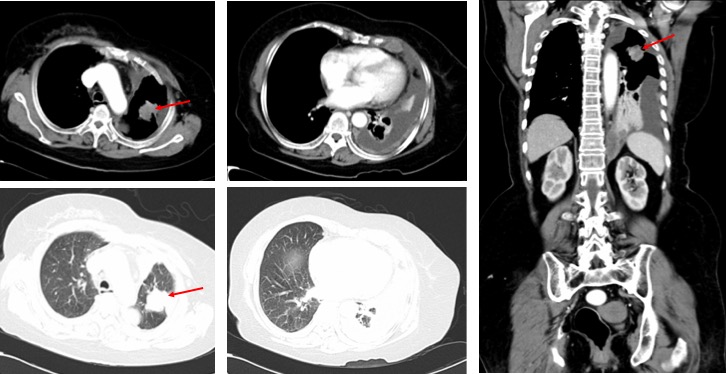
Diagnosis: Cerebral metastasis from lung carcinoma (HPE proven)
Discussion:
- Brain lesions in patients with known malignancies are usually suspicious for metastasis.
- The usual appearance on imaging is well-circumscribed lesion with enhancement and surrounding vasogenic oedema. On MRI the lesions are hypointense on T1 and hyperintense on T2/FLAIR sequences.
- The lesions are hypervascular and shows increased cerebral blood volume on perfusion imaging.
- Cystic metastasis have been described in carcinomas of the thymus, breast, prostate, lung and pancreas.
- However, cystic lesions are more commonly seen in brain abscesses, primary cerebral tumours or parasitic infection, especially in patients without history of malignancy.
- Diffusion weighted images may be helpful to differentiate cystic cerebral metastasis with cerebral abscess. However it may be false positive in hemorrhagic metastasis or when therapy has been started or in a fungal abscesses. MRS may be helpful with amino acid peak at 0.9 ppm is usually seen in pyogenic abscesses.
Recent Comments