Case contribution: Dr Radhiana Hassan
Clinical:
- A 46 years old lady
- Nulliparous
- Presented with sudden onset of severe LIF pain for 2 days
- Spontaneously resolved
- No per vaginal or per rectal bleed
- No bowel symptoms
- Colonoscopy normal
- Ultrasound showed cystic lesion at left flank
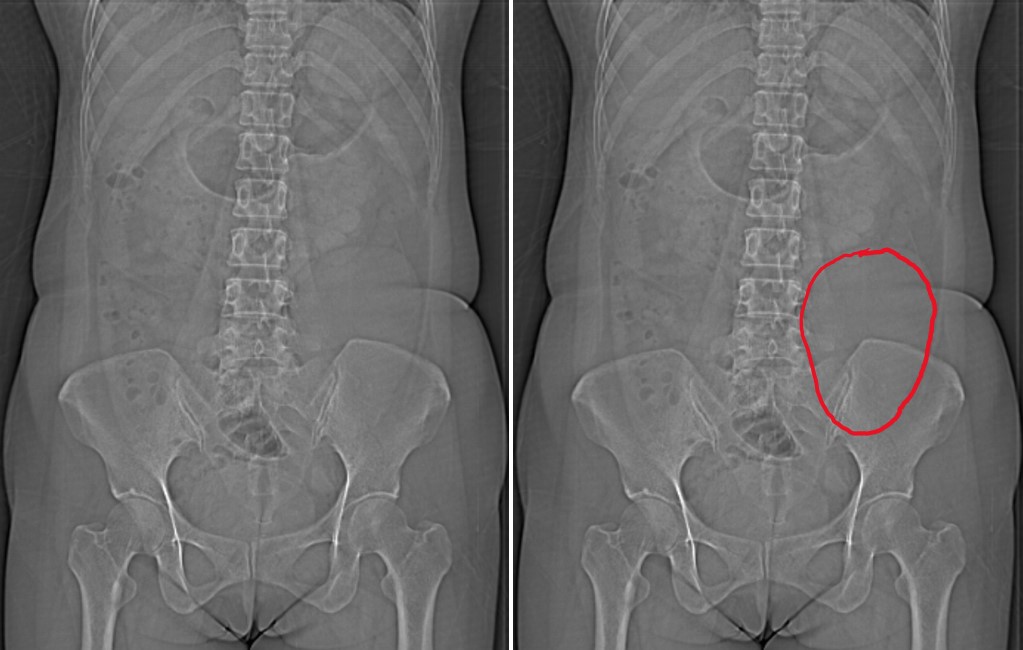
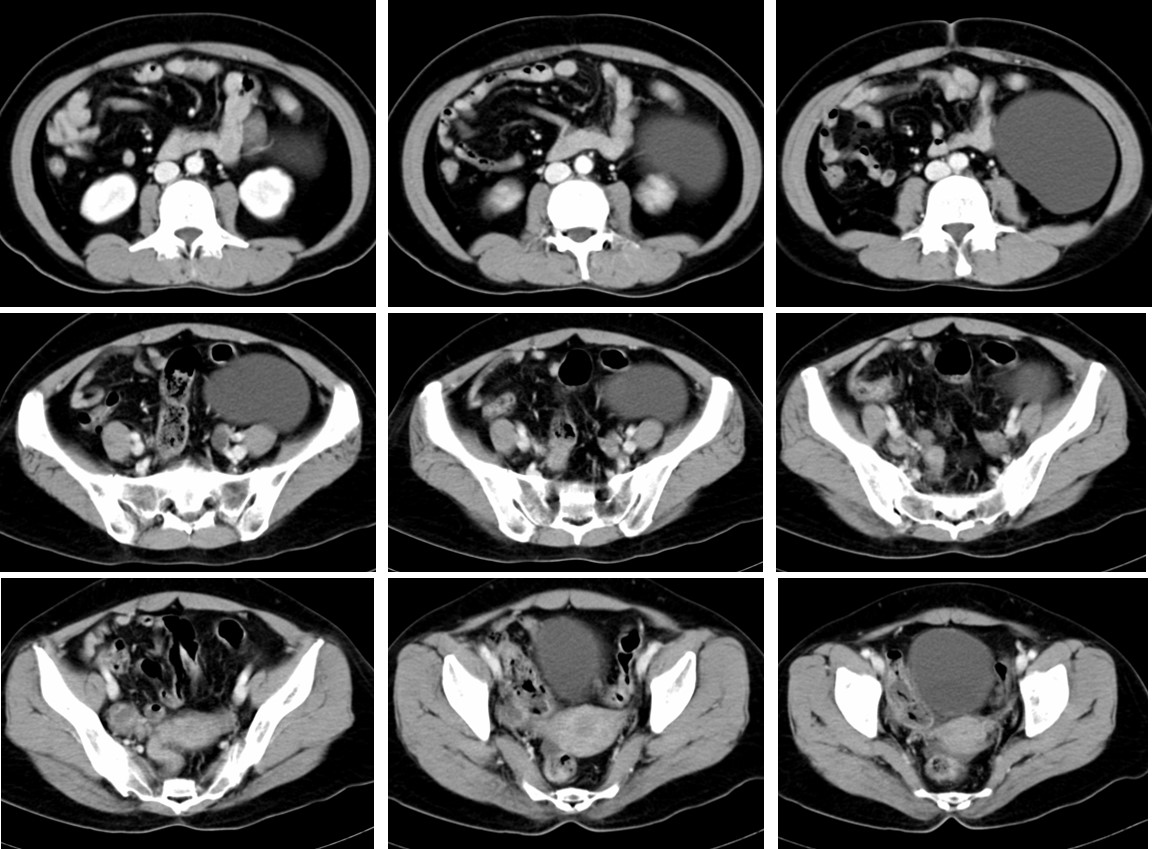
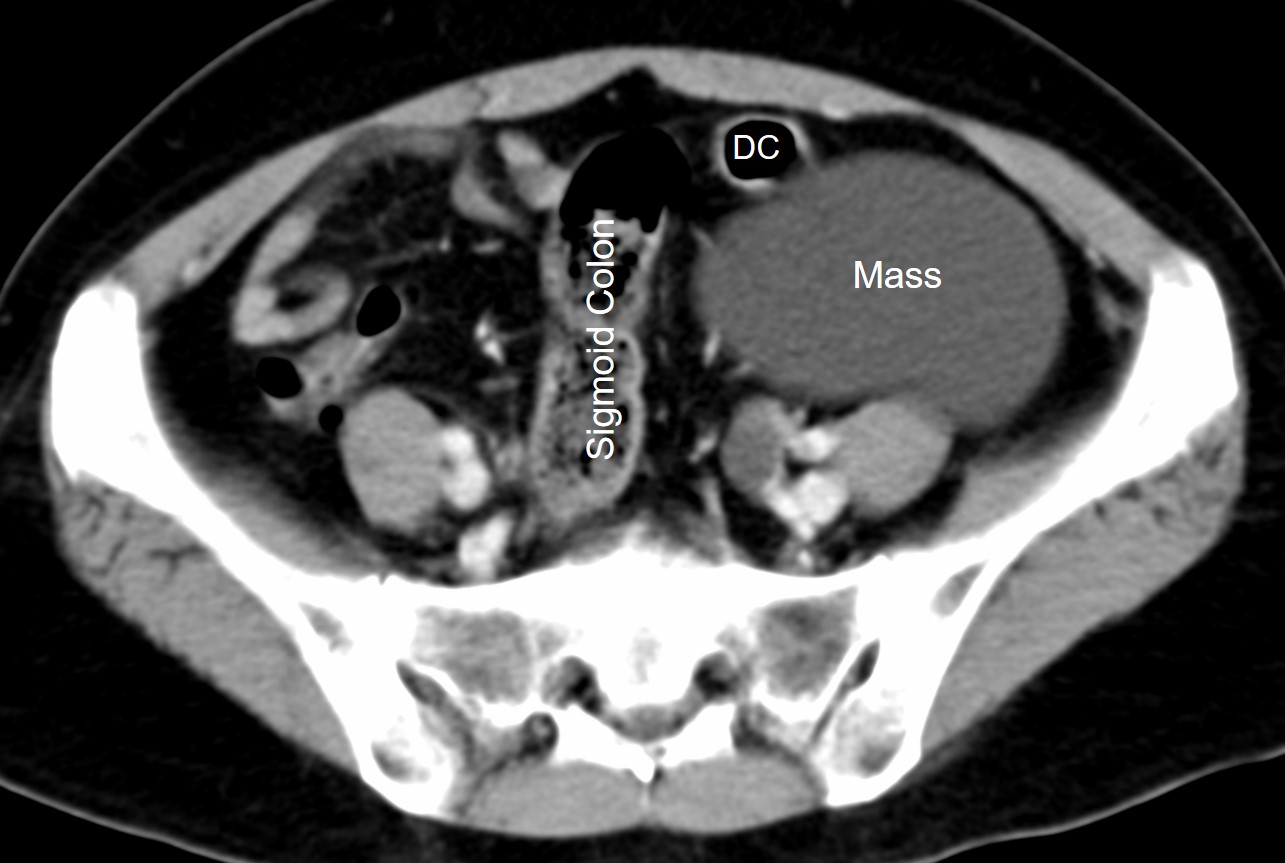
CT Findings:
- A well defined oval hypodense lesion at left lumbar region measuring about 9.3 cm x 3.8 cm.
- Density consistent with fluid.
- No calcification within the lesion.
- No septae.
- No solid component.
- Displaces the descending colon (DC) anteriorly
Intra-operative findings:
- A left retroperitoneal mesenteric cyst.
- Cyst arising from descending mesocolon
- The cyst is benign looking
- Uterus, fallopian tubes and ovaries are normal.
- Colon, small bowel, stomach, liver, gall bladder are normal
- Pelvic cavity normal, no adhesion
Histopathological findings:
- Macroscopy: specimen labelled as descending colon cyst consists of a cyst measuring 135x100x80 mm and weighing 500 gm. Cut section shows a unilocular cyst containing serous fluid. The wall is about 1 mm in thickness.
- Microscopy: section of the cyst wall shows to be lined by ciliated pseudostratified epithelium. There is no cytological or architectural atypia.
Diagnosis: Benign mesenteric cyst.
Discussion:
- Mesenteric cysts are rare, reported incidence of 0.5-1 per 100,000 admissions
- a very rare cause of abdominal pain
- have wide range of underlying causes
- It can occur anywhere in the mesentery, from the duodenum to the rectum and may extend into the retroperitoneum.
- The pathologic features vary considerably. They can be single or multiple, unilocular or multilocular; they can have serous, chylous, hemorrhagic, or mixed fluid contents; and their lining can vary from a flattened endothelial monolayer to a cuboidal or columnar epithelium to patchy fibrosis.
- Rarely the cyst wall contains calcium
- Differential diagnosis: ovarian cyst, pancreatic pseudocyst, meconium pseudocyst, urachal cyst, peritoneal hydatidosis
- The case illustrate the importance to document the origin of the lesion, extent and the nature of the cystic mass in the abdomen.
Progress of patient:
- As initial diagnosis was an ovarian cyst, patient was operated by O&G team
- On-table referral was done to surgical team
- Patient had uneventful post operative recovery
- Discharged well
Recent Comments