
Clinical:
- A 45 years old lady with no known underlying medical illness
- Presented with progressive numbness of bilateral lower limb for one year.
- She also had progressive loss of motor power for the past 3 months.
- There was no associated constitutional symptom.
- Clinically loss of power and sensation noted at the level of T6.

MRI findings:
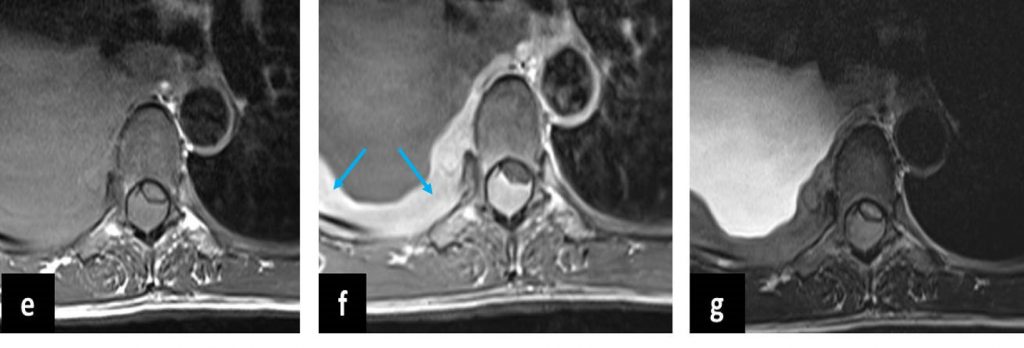
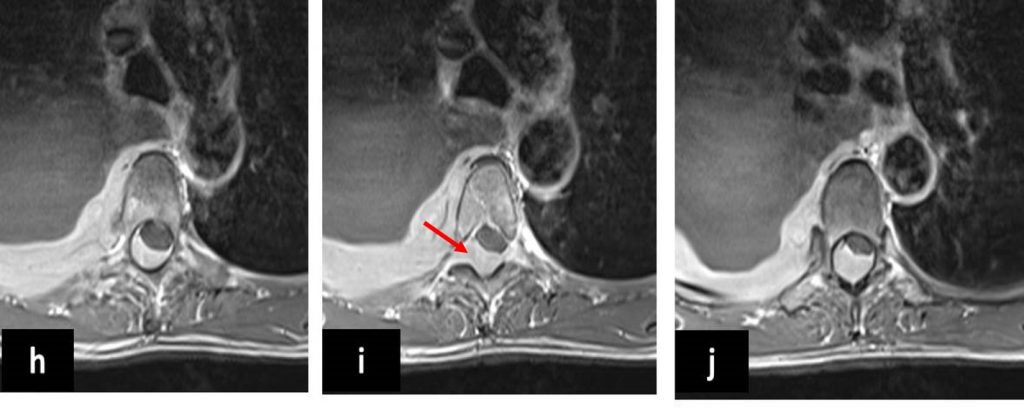
- It showed an intraspinal epidural mass (yellow arrows) which is isointense to spinal cord on T1 and T2-weighted images with marked homogenous enhancement on post contrast images.
- The mass displaces the cord to the left side and anteriorly.
- There is right neural foramina extension (red arrow) to the right paravertebral and retrocrural region.
- Abnormal bone marrow signal (blue block arrows) of a few thoracic vertebrae is also seen.
- This patient also had right pleural effusion (blue arrows) .
- CT thorax and abdomen showed no other lesion except the effusion (images not shown).
Diagnosis: B-cell lymphoma (HPE proven).
Discussion:
- An epidural location of lymphoma is observed in 0.1-6.5% of all lymphomas.
- Patient clinically present most commonly in the fifth to seventh decade of life with more than 80% being older than 40 years.
- Thoracic spine is most commonly involved and has been reported in 75% of cases.
- Symptoms occur due to spinal cord and nerve root compression. Within the spinal canal, the location of the tumour is usually dorsal than ventral.
- MRI appearance is isointense on T1-weighted images, iso to hyperintense on T2-weighted images with marked contrast enhancement.
- Mean longitudinal extension of the lesion was 2.6 vertebral bodies.
- In majority of patients, diffuse changes in vertebral body marrow were seen adjacent to or at distance from the lesion.
- Cortical destruction or vertebral collapsed is rarely seen.
- The differential diagnoses include tuberculous spondylitis, epidural abscess, metastasis and malignant peripheral nerve sheath tumours.
Recent Comments