
Clinical:
- A 12 years old girl
- Presents with neck pain, loss of appetite and loss of weight for two week.
- Worsening of the symptoms three days prior to presentation.
- There was no history of fever, trauma or dysphagia.
- Clinically there is no neurological deficit.
Imaging findings:
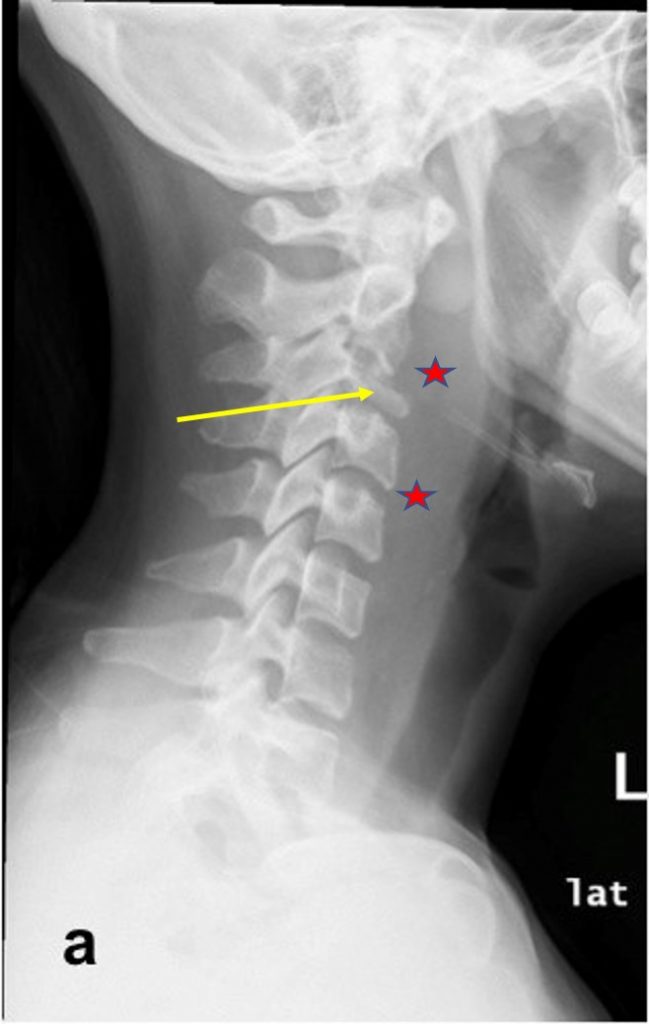
- Cervical radiograph in lateral projection (a) shows loss of normal cervical lordosis with significant reduction of C3 vertebral body height (yellow arrow).
- There is associated with prevertebral soft tissue thickening (red stars)
- No air pocket was seen within the soft tissue.
- The intervertebral disc spaces were intact.
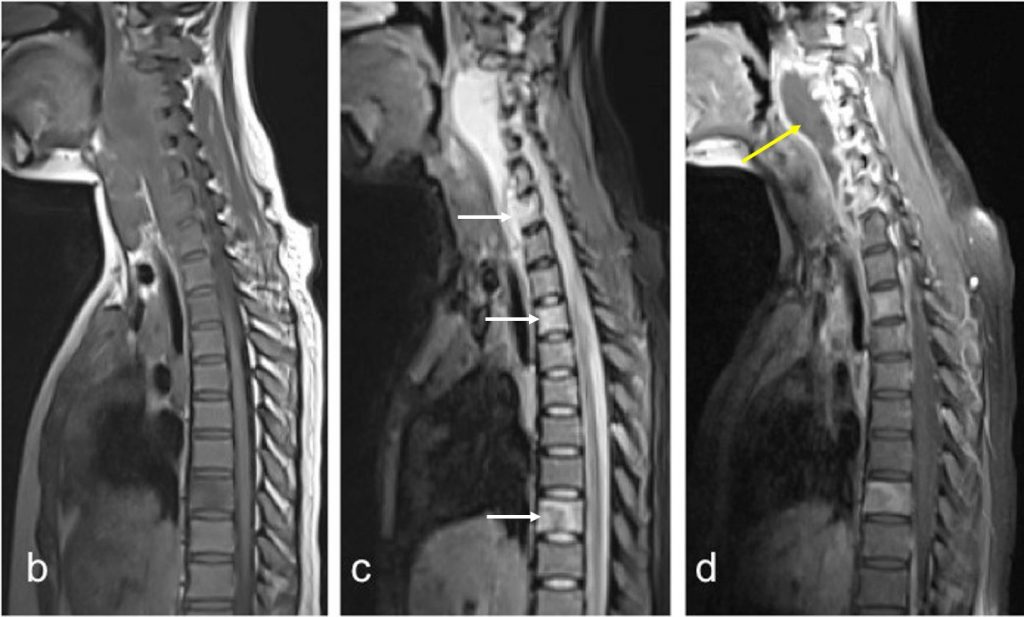
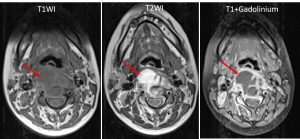
- On sagittal MRI of the spine, (b) T1WI, (c) T2WI and (d) T1-post contrast, multiple cervical vertebrae involvement is demonstrated (white arrows).
- A preverterbal collection with rim enhancement is seen (yellow arrow).
- There is subligamentous spread inferiorly with intraspinal extradural extension.
- Relative sparing of the intervertebral discs with skip lesion at lower thoracic vertebra was also demonstrated.
Diagnosis: Tuberculous spondylitis (HPE proven).
Discussion:
- Tuberculous spondylitis refers to vertebral body osteomyelitis and intervertebral diskitis from tuberculosis.
- Tuberculous spondylitis typically begins in the anterior aspect of the vertebral body adjacent to the disc.
- The infection then spread to the adjacent vertebral bodies under the longitudinal ligaments.
- Spread to the surround soft tissue to form paravertebral abscesses occur frequently.
- Non-contagious skip lesions are also seen.
- The most frequent site of spinal tuberculosis is the thoracolumbar junction. However, any segment of the spine can be involved and many levels may be involved at presentation.
- Radiographical findings include narrowing of the intervertebral disc spaces, adjacent end-plate irregularity and erosion, sequestrate and paravertebral masses.
- It is difficult to differentiate TB spondylitis from pyogenic spondylitis based on radiograph and correlation with clinical and social history is necessary.
- Computed tomography (CT) scan can clearly demonstrate bony sclerosis and destruction. Epidural abscesses, bony fragmentation and spinal canal compression can also be seen.
- MRI can detect changes within the vertebra and end-plate irregularity earlier than radiograph and bone scan. It is the modality of choice to evaluate the soft tissue extension. It is also sensitive to detect marrow changes of vertebral osteomyelitis.
Recent Comments