
Clinical:
- A 33 years old lady
- Non-smoker
- Presented with chronic cough and recent onset of shortness of breath
- Associated with constitutional symptoms
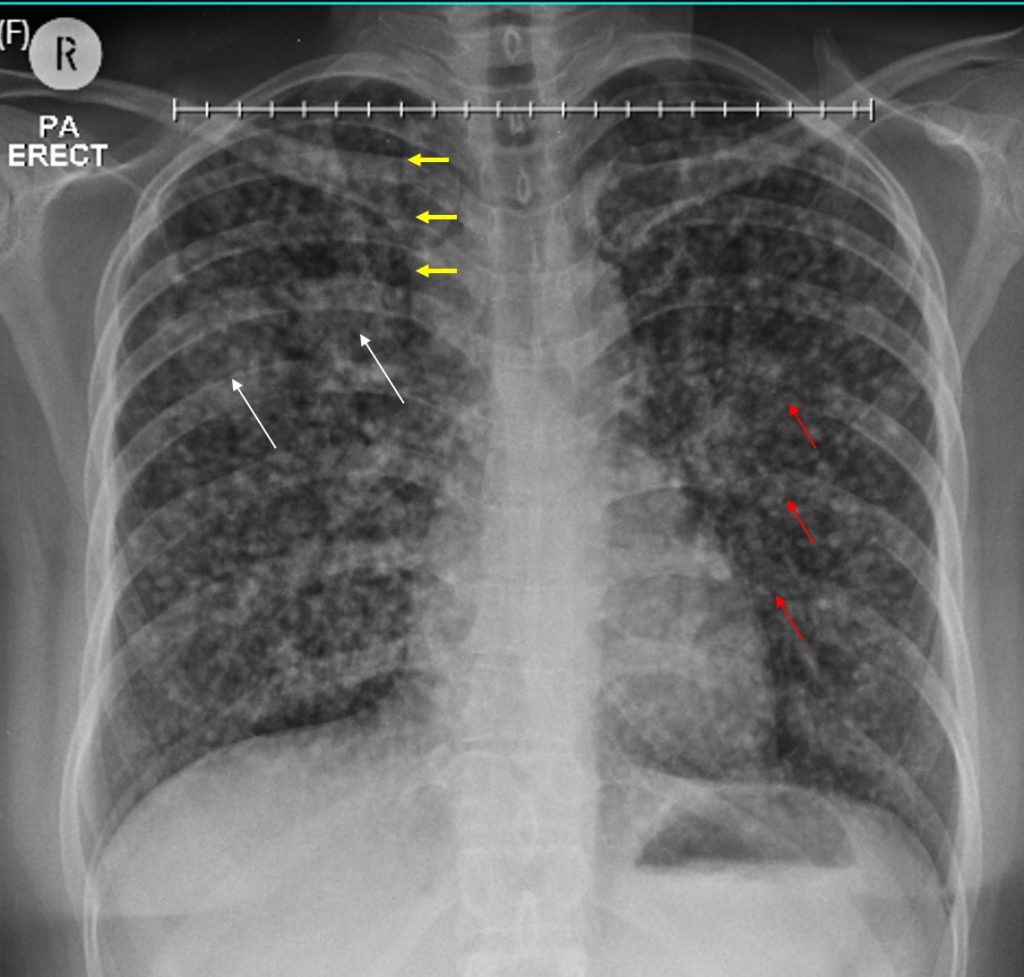
Radiographic findings:
- Numerous small nodular opacities are seen in both lung fields.
- Some confluent areas are seen at right upper zone and perihilar region (white arrows).
- Prominent right paratracheal stripe (yellow arrows).
- Loss of cortical outline of 7th to 9th posterior ribs on the left side (red arrows) suggestive of lytic destruction of bones.
- No pleural effusion or pneumothorax.
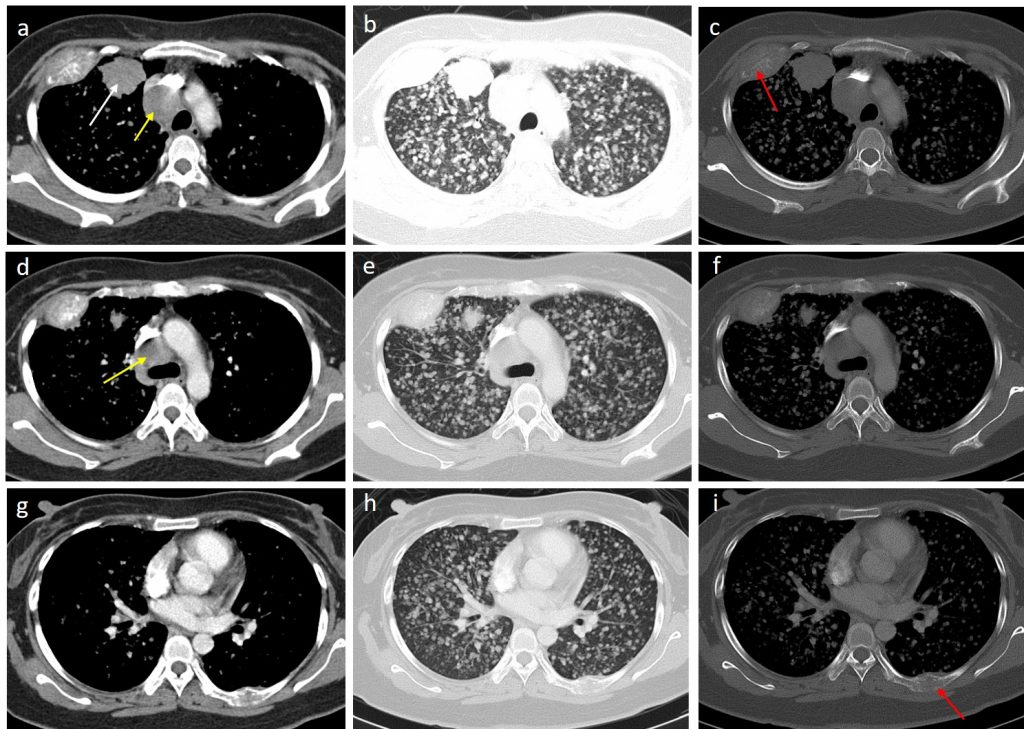
CT findings:
- A lobulated mass is seen in the anterior segment of right upper lobe measuring about 34 mm (white arrow). No calcification or necrotic region within. No cavitation within the lesion.
- There are numerous nodules with generalized distribution in all segments of both lung fields. The nodules are well-defined and almost similar in size.
- No consolidation, bronchiectasis or septal thickening seen.
- No pleural thickening or abnormal pleural enhancement. No pneumothorax or pleural effusion.
- There are multiple enlarged mediastinal nodes. The largest involving the upper and lower paratracheal nodes measuring 30 mm and 18 mm respectively (yellow arrows). The enlarged paratracheal nodes are causing mass effect causing anterior displacement and narrowing of proximal SVC. The distal SVC is normal.
- There are lytic destructions of the ribs seen. The largest lytic lesion of anterior 3rd rib on the right side seen with surrounding soft tissue measures about 57 mm. Another lesions involving left 7th and 8th posterior ribs.
HPE findings:
- Macroscopy: specimen labelled as right upper lobe mass consist of whitish strip of white tissue.
- Microscopy: levels show multiple strips of fibrocollagenous tissue harbouring malignant tumour arranged as crowded and irregular glands. These glands are lined by moderately pleomorphic tumour cells, having ovoid vesicular nuclei and some have prominent nucleoli. Abnormal mitosis is identified. Intraluminal necrosis is also seen. No squamous differentiation noted.
Diagnosis: Lung adenocarcinoma
Discussion:
- Adenocarcinoma represents 31% of all lung cancers,
- Increasing numbers of non‐smokers and never‐smokers are seen developing lung adenocarcinoma
- Lung adenocarcinoma has a spectrum of appearances on CT, many of which mimic non‐malignant processes.
- Multifocal lung adenocarcinoma is less common than solitary adenocarcinoma.
- The tumours may be found in a single lobe of the lung, multiple lobes of one lung or multiple lobes of both lungs.
- The lesions are often at different stages along the adenocarcinoma spectrum, potentially giving rise to different appearances of adenocarcinoma within the single patient.
- Hila or hila and mediastinal involvement is seen in 51% of cases on chest radiography.
Recent Comments