
Clinical:
- A 70 years Indian man
- Chronic smoker and tobacco-chewing for many years
- Presented with whitish-red lesion at left buccal mucosa
- Clinically a shallow ulcer seen in the middle of the lesion about 3×3 mm, oval in shape
- Biopsy done
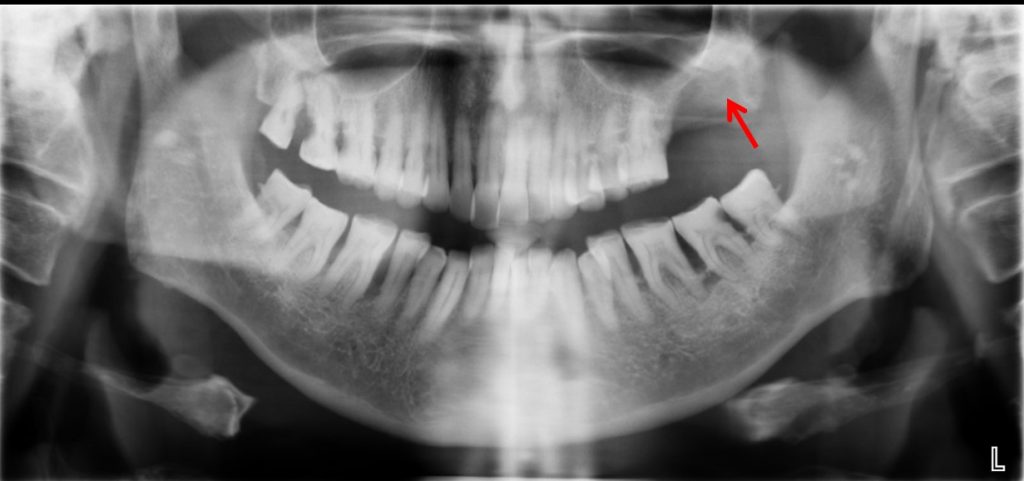
Radiographic findings:
- A lytic lesion seen at left maxillary bone (red arrow)
- It shows fairly well-defined border
- No sclerotic margin
- No obvious soft tissue mass
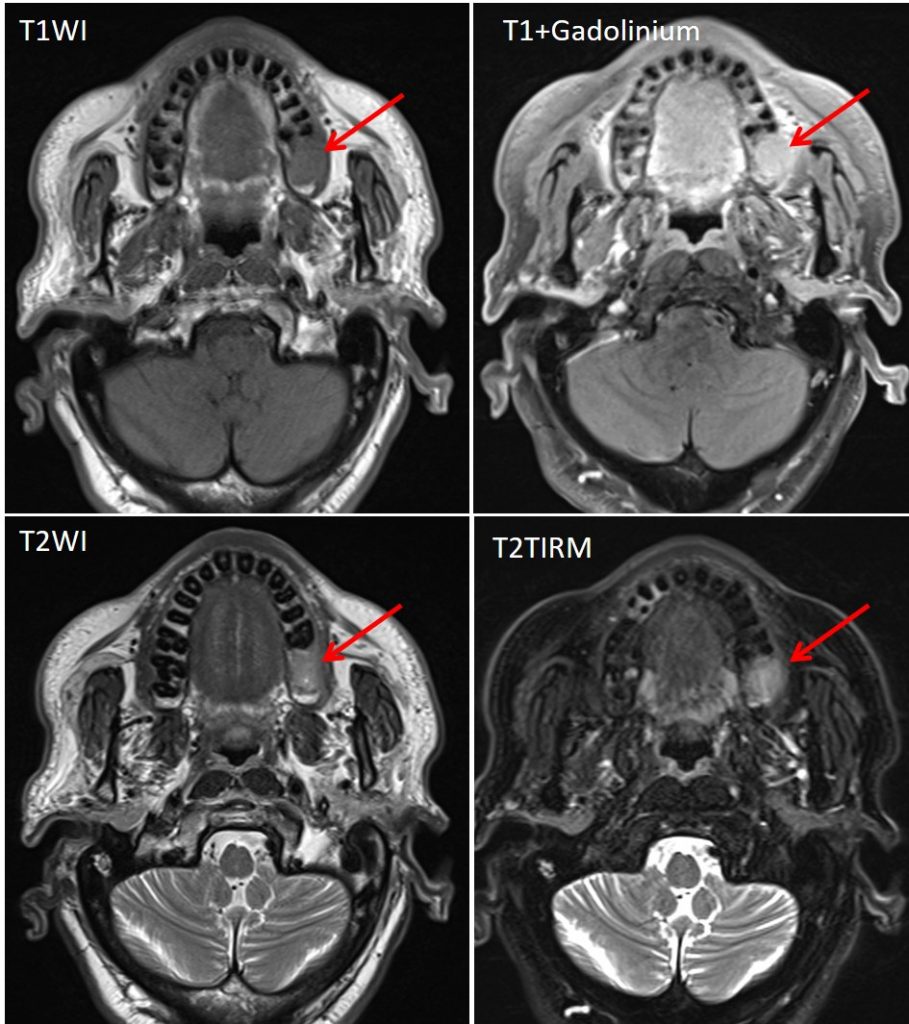
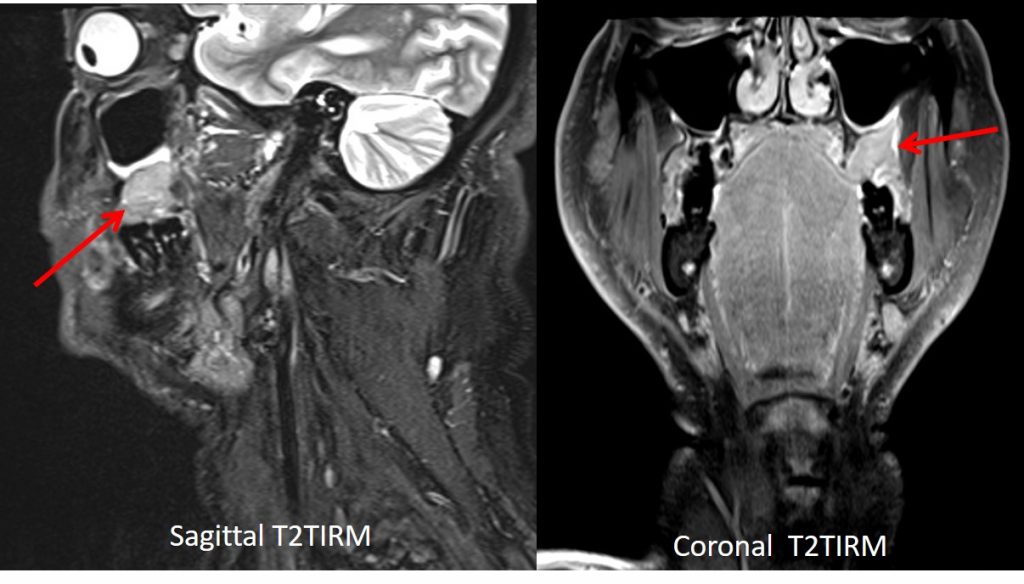
MRI findings:
- There is a lobulated lesion in the superior left alveolar process of maxilla adjacent to left 1st molar, measuring approximately 1.2 x 1.6 x 2.1 cm (AP x W x CC).
- This lesion is isointense to the adjacent muscle on T1, hyperintense on T2 and not suppressed on TIRM. Mild enhancement is present on post IV contrast.
- The lesion seen extending along the alveolar process posteriorly and causes erosion of outer cortex of mandible.
- Medially the inner cortex of affected mandible is still preserved.
- This lesion extends to the adjacent buccal mucosa, however the buccinator and pterygoid muscle are preserved.
- There is suspicious extension into the left retromolar trio trigone region.
- No extension into the left maxillary sinus. The soft and hard palate are preserved. The left carotid artery is not involved. The uvula is unremarkable. The submandibular, sublingual and parotid gland appears normal.
HPE findings:
- Macroscopy: specimen labelled as soft tissue from left buccal mucosa
- Microscopy: The section shows malignant epithelial cells arising from dysplastic parakeratinized stratified squamous epithelium and invading the underlying connective tissue in sheets, islands, cords and nests. These tumour cells demonstrate cellular and nuclear pleomorphism, increased nuclear to cytoplasmic ratio, dyskeratosis, prominent nucleoli and interbridging. Keratin production is moderate. Mitosis is minimal. Stromal reaction consists of dense chronic inflammatory cell infiltrate
- Interpretation: squamous cell carcinoma, well-differentiated.
Diagnosis: Buccal mucosa SCC
Discussion:
- Squamous cell carcinoma (SCC) accounts for vast majority (90%) of malignancies of the oral cavity.
- Spread of oral SCC occurs via (a) direct extension over mucosal surfaces, muscle and bone, (b) by dissemination via lymphatic drainage and (c) by extension along neurovascular bundles
- The presence of osseous involvement is indicative of a T4 lesion
- Subtle cortical erosions are best detected with CT scan whereas the extent of marrow involvement is better assessed using MRI
- Evidence of osseous involvement seen at imaging precludes a wide local excision during surgical treatment.
- TNM classification for primary tumour of oral cavity:
- Tx: primary tumour cannot be assessed
- T0: no evidence of primary tumour seen
- Tis: primary tumour is carcinoma in-situ
- T1: primary tumour has a maximal diameter of 2 cm or less
- T2: Primary tumour has a maximal diameter of more than 2cm but not more than 4 cm
- T3: primary tumour has a maximal diameter of more than 4 cm
- T4a: primary tumour involves cortical bone, intrinsic or extrinsic muscle of the tongue, maxillary sinus or skin
- T4b: primary tumour involves masticator space, pterygoid plates, skull base and internal carotid artery
Recent Comments