
Clinical:
- A 67 years old man
- Underlying history of colon carcinoma
- Right hemicolectomy done 2 years ago for adenocarcinoma of ascending colon, T4aN2aM1
- Presented with acute abdominal pain and distension
- History of chronic constipation for the past one month

Radiographic findings:
- There are dilated bowel loops
- These dilated bowel loops are centrally located
- Valvulae conniventes aer seen crossing the width of the dilated bowel loops (white arrows)
- ‘stack of coin’ appearance also seen (block arrow)
- No obvious free air
Radiologic diagnosis: Small bowel obstruction
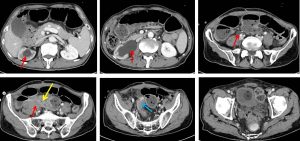
CT scan findings:
- There is a soft tissue enhancing mass at right iliac fossa region measures about 2.9 x 4.0 cm in size (yellow arrow).
- No clear plane of demarcation with the adjacent right external iliac artery, which is partially encased within the mass.
- The adjacent sigmoid colon is retracted into the mass with poor plane of demarcation seen (blue arrow). There are also associated circumferential bowel wall thickenings seen within the sigmoid colon with some luminal narrowing.
- Gross right hydronephrosis and hydroureter (red arrows) seen. The grossly dilated right ureter is abruptly terminated around the bowel mass, likely infiltrated within the mass.
- There are also associated gross dilatations of the small bowels proximal to the mass indicating a near total obstruction.
- Air fluid levels also seen within the dilated small bowels.
- The descending colon and part of the transverse colon is normal.
Discussion:
- Small bowel are dilated if calibre of proximal jejunum > 3.5 cm, mid small bowel >3.0 cm and ileum > 2.5 cm
- Small bowel dilatation with normal mucosal folds can be due to mechanical obstruction (adhesions, strangulated hernia), paralytic ileus, coeliac disease, scleroderma or iatrogenic causes.
- Signs of small bowel obstruction on radiograph include centrally located dilatation of bowel loops, involving several dilated loops, visualization of valvulae conniventes, stack of coin appearance and fluid levels on erect films.
Progress of patient:
- Exploratory laparotomy, adhesiolysis and loop ileostomy performed
- Intra operatively noted to have dilated small bowels
- Tumour recurrence at right iliac fossa region with small bowel, large bowel and posterior wall stuck together
- Dense adhesion noted at distal jejunum about 30 cm from DJ junction causing closed loop obstruction
- Patient was discharged well
Recent Comments