
Clinical:
- A 38 years old lady
- Presented with fullness at suprapubic region
- Gradual increase in size
- No other symptoms
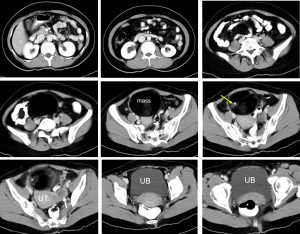
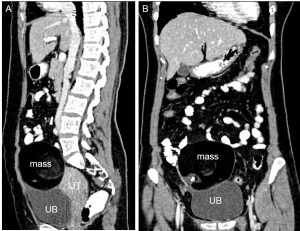
CT scan findings:
- There is a well-defined rounded mass measuring about 10x10x8 cm
- The mass is located superior and to the right side of uterus and urinary bladder most likely arising from right ovary.
- It shows mixed density with predominant fat component.
- Presence of calcification seen
- Minimal solid component which shows no enhancement post contrast
- No ascites, no local infiltration
- The left ovary and uterus are grossly normal
Intraoperative findings:
- Operation done one year after the CT scan
- Right ovarian cyst, benign looking 10×8 cm, solid cystic twisted x2
- Left ovary normal
- No ascitic fluid
HPE findings:
- Macroscopy: specimen labelled as right ovarian cyst consists of a rounded hard ovary measuring 10x60x30 mm, weighing 400 gms. The external surface is smooth. There is no haemorrhage or adhesion noted. There are two small cysts on the surface of the ovary measuring 5×3 mm and 5×5 mm respectively. On cut section, there is wall like material with hairs.
- Microscopy: sections of the fibrous cyst wall shows to be lined by predominantly flattened cuboidal cells. Also noted sebaceous glands and hair shafts. Some multinucleated giant cells are also seen. Focal area of adipose tissue noted. No immature element
- Interpretation: Right ovarian cyst compatible with benign cystic teratoma
Diagnosis: Ovarian mature cystic teratoma
Discussion:
- Mature cystic teratomas also known as “dermoid cysts”
- It is cystic tumor composed of well-differentiated derivations from at least two of the three germ cell layers (ectoderm, mesoderm, and endoderm).
- They affect a younger age group (mean patient age, 30 years) than epithelial ovarian neoplasms
- Most mature cystic teratomas are asymptomatic. Abdominal pain or other nonspecific symptoms occur in the minority of patients.
- The tumors are bilateral in about 10% of cases.
- Ultrasound features are variable. The most common finding is a cystic lesion with a densely echogenic tubercle (Rokitansky nodule) projecting into the cyst lumen. The second manifestation is a diffusely or partially echogenic mass with the echogenic area usually demonstrating sound attenuation owing to sebaceous material and hair within the cyst cavity. The third manifestation consists of multiple thin, echogenic bands caused by hair in the cyst cavity. Pure sebum within the cyst may be hypoechoic or anechoic. Fluid-fluid levels result from sebum floating above aqueous fluid, which appears more echogenic than the sebum layer. The dermoid plug is echogenic, with shadowing due to adipose tissue, calcifications or hair arising from it.
- The diagnosis of mature cystic teratoma at CT and MR imaging is fairly straightforward because these modalities are more sensitive for fat. At CT, fat attenuation within a cyst, with or without calcification in the wall, is diagnostic for mature cystic teratoma. Fat is reported in 93% of cases and teeth or other calcifications in 56%.
- Complications of mature cystic teratoma include rupture, malignant degeneration, or (most commonly) torsion.
- Mature cystic teratomas affected by torsion are larger teratomas. Findings suggestive of torsion include deviation of the uterus to the twisted side, engorged blood vessels on the twisted side, a mass with a high-signal-intensity rim on T1-weighted MR images, a low-signal-intensity torsion knot, and thick, straight blood vessels that drape around the mass and cause complete absence of enhancement.
Recent Comments