
Clinical:
- A 28 years old lady
- History of irregular menses and dysmenorrhoea
- Presented with fullness at suprapubic region
- Ultrasound showed a complex ovarian cyst
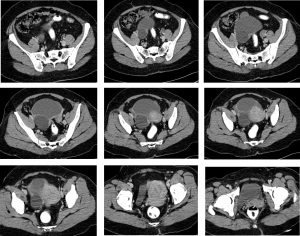
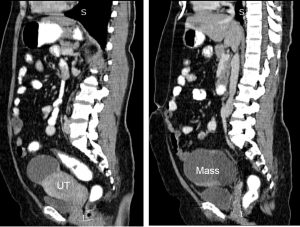
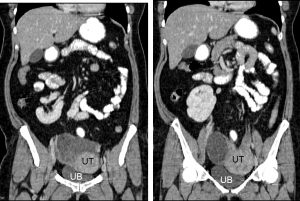
CT scan findings:
- Cystic lobulated mass at right side of pelvis measuring 10x10x10 cm
- It shows thick wall, mild enhancement of the wall post contrast, presence of septae also noted
- No calcification, no fat component
- No ascites
Intra-operative findings:
- Right ovarian cyst, thickened capsule adhered to the descending colon, sigmoid colon, caecum and rectum. Also adhered to right lateral pelvic wall, dense adhesion at POD stuck to the back of the uterus. Size 8x6x6 cm, removed intact. Opened up, no chocolate material within the cyst
- Left ovary stuck to the back of the uterus as well, encased in the dense adhesion between the descending and sigmoid colon and back of the uterus. Removed separately
- Bilateral hydrosalphinges.
- Multiple endometriotic spots sene on the anterior uterine wall and uterine fundus, new lesion and burnt out lesions.
- Omentum adhered to right ovarian cyst
- No palpable node
HPE findings:
- Macroscopy: specimen consists of a uterus, both fallopian tubes, right ovarian cyst and left ovary. The left ovary is separated from the main specimen. The left ovary measures 25x30x10 mm. Cut section of left ovary shows corpus luteum. The right ovarian cyst measures 35x45x15 mm and is partially ruptured. Multiloculated cyst with a wall thickness of 2 to 20 mm. The outer surface is irregular, the inner surface is smooth with focal yellowish discolouration. No necrosis, papillary structures or nodules seen.
- Microscopy: Sections show a tubo-ovarian cystic lesion lined in many areas by a flattened epithelium as well as endometrial epithelium with stroma included in some areas. Foci of endometrial tissues are seen on the serosa of the right fallopian tube. The endometrium is suboptimally presented but is in proliferative phase. The cervix, left ovary and fallopian tube show no significant pathology.
- Diagnosis: endometriosis of right ovary and fallopian tube
Diagnosis: Ovarian endometrioma.
Discussion:
- Endometriomas, also known as chocolate cysts or endometriotic cysts.
- It affects women during the reproductive years and may cause chronic pelvic pain associated with menstruation.
- The ovaries are involved in approximately 75% of patients with endometriosis.
- Other locations include: cul-de-sac, posterior broad ligament, uterosacral ligaments, uterus and colon.
- On ultrasound endometrioma can be variable but the great majority (about 95%) of patients present with a classic homogeneous, hypoechoic cyst with diffuse low level echoes.
Endometriomas can be multilocular and have thin or even thick septations. - If additional imaging is needed, it is better to perform MRI.
On T2-weighted images endometriomas typically show ‘shading’. MRI can confirms the absence of enhancement. On MRI the hemorrhagic content will make endometrioma appear bright on T1-weighted images. On T1-fatsat images an endometrioma will remain bright. This in contrast to teratomas, that are also bright on T1 but dark on T1-fatsat images.
Recent Comments