")
Clinical:
- A 73 years old man
- Underlying HPT and gouty arthritis
- Presented with mass at right leg for 5 months
- Initially started with redness at medial aspect of right leg, no trauma or other known precipitating factor
- Worsening and become swelling
- Progressive increase in size, now about size of an egg
- No night pain, does not disturb ambulation and joint movement
- Had associated LOA and LOW
- No other swelling at other part of body, no fever
- Clinical examination shows mass at medial aspect of distal leg with prominent veins. The lesion measures 10×10 cm. No skin ulceration, no fungating mass, no discharge, non tender, fixed and attached to skin and underlying structure. No palpable bruit. No enlarged inguinal node. Sensation and muscle power are normal.
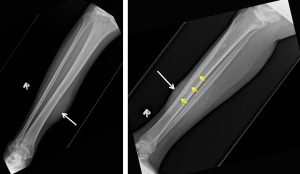
Radiographic findings:
- Soft tissue swelling seen at anteromedial part of the right leg (white arrow)
- Homogenous opacity with no calcification within it.
- No lucent area within to suggest presence of air.
- The overlying skin looks normal.
- There is smooth thickening of the anterior cortex of right tibia. No permeative bone changes, no fracture or other type of periosteal reaction.
HPE findings:
- Macroscopy: specimen labelled as soft tissue consist of whitish strips measuring 15-22 mm in length
- Microscopy: sections show diffuse proliferation of atypical cells reminiscent starry-sky appearance. The cells are large with vesicular nuclei and prominent nucleoli. The cytoplasm is scanty. Apoptotic bodies and mitosis are frequently seen. Intermingle reactive T-lymphocytes are present. There is no overlying skin or bony tissue in this biopsy. Area of necrosis is also seen.
- Immunohistochemical staining: CKAE1/AE3, CD3 are negatives. LCA/CD45, diffusely positive, CD10 positive and Ki67 High (80%).
- Interpretation: Features are suggestive of diffuse large B cell lymphoma, germnal centre subtype.
Progress of patient:
- BMAT: apart from slight increase in eosinophils and its precursors, the marrow aspirate is relatively normal. No evidence to suggest marrow infiltration by abnormal lymphoid cells. There is no significant presence of plasma cells to suggest multiple myeloma.
- CT scan thorax, abdomen and pelvis shows no abnormal enlargement of lymph nodes. Visceral organs are normal. No lung nodules.
- Patient was referred to hematologist and oncologist in another hospital for further treatment.
Final diagnosis: Primary lymphoma of soft tissue (leg)
Discussion:
- Malignant lymphoma of soft tissue is extremely rare. Travis et al showed that among 7000 malignant lymphomas, only 8 (0.11%) were soft tissue malignant lymphomas.
- In the literature, several case reports and case series of soft tissue malignant lymphoma have been reported.
- Soft tissue lymphoma can develop in any sites, but is common in the extremities.
- Lower limb involvement is more common compared to upper limb.
- In this case, the soft tissue swelling is not associated with skin changes or skin ulceration, suggesting soft tissue origin. However we cannot determine whether the lymphoma is soft tissue lymphoma or skin lymphoma (which is more common). If it is categorized as skin lymphoma, the diagnosis would be DLBCL, leg type.
Recent Comments