
Clinical:
- A 50 years old lady
- Abdominal distension for many months
- No constitutional symptoms
- No bowel related changes
CT scan findings:
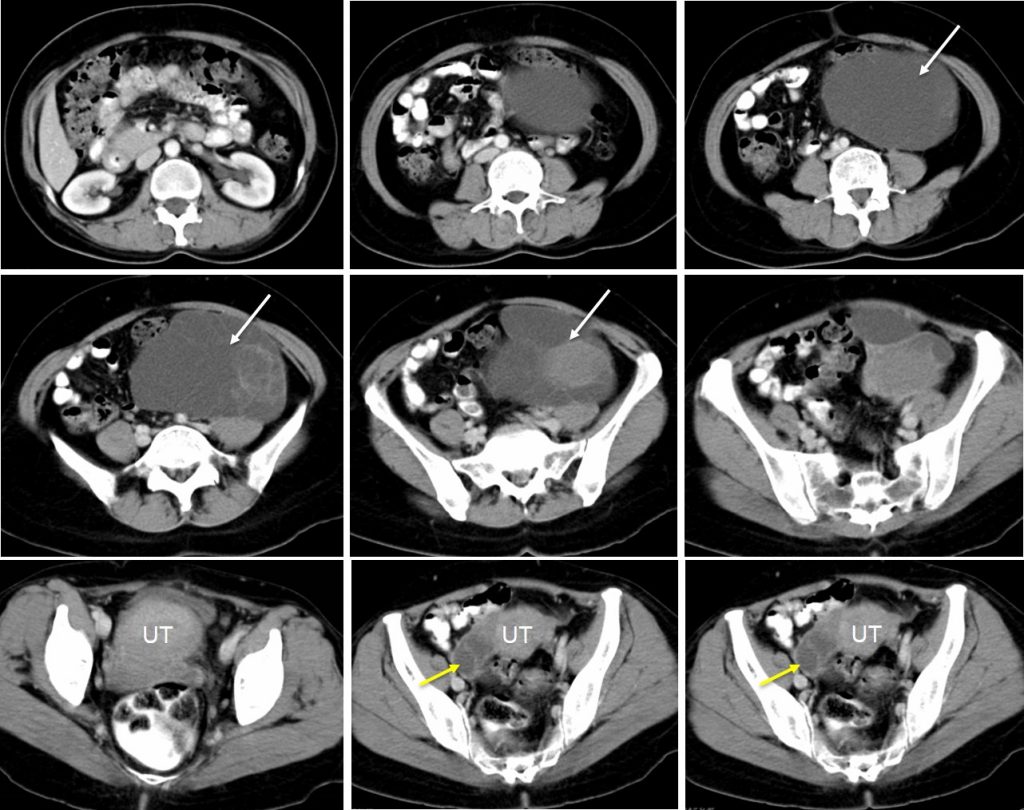
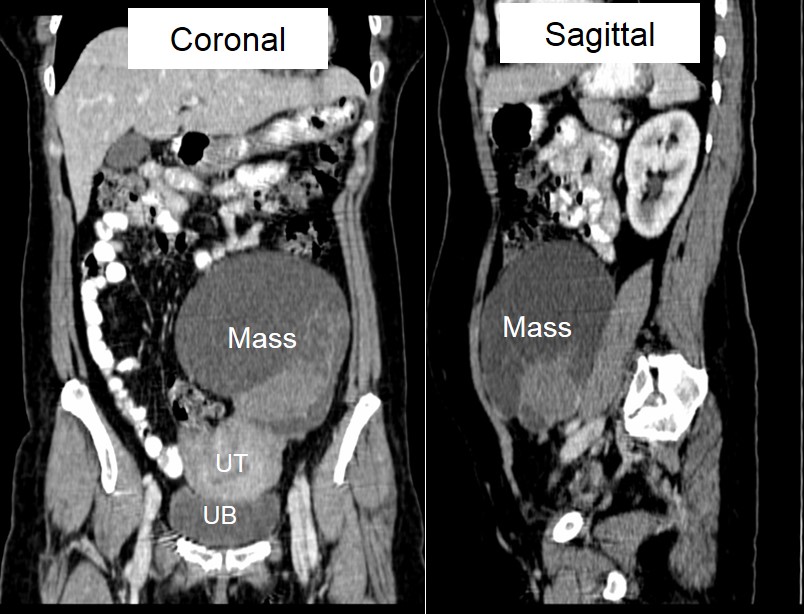
- A large heterogenous mass arising from left side of pelvis, likely ovarian in origin measuring about 13x12x9 cm (white arrows). The mass is predominantly cystic with multiple septation within. Presence of solid component in its inferior pole which enhances post contrast. The cyst wall is thin and abut the adjacent structures.
- Another lesion at right ovary measuring 4x4x2 cm which has thick wall and septations (yellow arrows).
- No calcification within the two cysts.
- No evidence of bowel or urinary obstruction.
Intra-operative findings:
- Left ovarian tumour measuring 15×15 cm mixed solid and cystic which ruptured during manipulation. Dense adhesion between the tumour and left side of pelvic wall, omentum and bowel. Dense adhesion also noted between posterior wall of uterus to the bowel.
- Uterus normal. No ascites
- Right ovary is normal.
HPE findings:
- Macroscopy: Specimen labelled as uterus, cervix, ovary and fallopian tubes. Right ovary and fallopian tube show no obvious abnormality. The left ovarian cyst consist of a lobulated brownish cystic lesion measuring 120x90x45 mm. It is a multiloculated cyst with locules ranging from 2 mm to 60 mm, some filled with clear gelatinous material and others containing brownish material. No solid area seen. The cyst wall is about 1 mm to 12 mm in thickness.
- Microscopy: Section of the cervix shows acute on chronic cervicitis with mild regenerative glandular hyperplasia. The endometrium is inactive. An occasional endometrial gland without stroma is seen deep within the myometrium. The right ovary has scattered cystic spaces lines by endometrial epithelium without endometrial stroma. The surrounding ovarian stroma is dense. The fallopian tube is unremarkable. The left ovarian cyst wall and locules are lined by tall, columnar, mucin-secreting epithelium. Mild focal tufting is seen but there is no multilayering, atypia, mitosis or invasion. A few cystic spaces lined by endometrial epithelium without endometrial stroma and surrounded by dense ovarian stroma is seen in a few areas.
- Interpretation: mixed mucinous cystadenoma and endometrioid cystadenofibroma of left ovary and early endometrioid adenofibroma of right ovary.
Diagnosis: Bilateral endometrioid cystadenofibromas of ovaries.
Discussion:
- Ovarian cystadenofibroma is a type of surface epithelial tumour.
- These tumours exhibit a fibrous stroma in variable amounts in all subtypes. When the stroma occupies an area greater than the cystic portion, the suffix “-fibroma” is added.
- The presence of more than 1 cyst over 1 cm in diameter warrants use of the prefix “cyst” as in “cystadenofibroma.”
- These tumours are classified, according to the epithelial cell types present, as serous, endometrioid, mucinous, clear cell, and mixed categories.
- The degree of epithelial proliferation and its relation to the stromal component of the tumour are the criteria used for the classification as benign, borderline, or malignant, although most of the reported ovarian cystadenofibromas were benign.
- When imaged by ultrasonography or CT, ovarian cystadenofibroma may appear as a complex solid and cystic mass and be difficult to differentiate from malignancy.
- MRI may be an essential modality for diagnosing this tumour, especially when the characteristic “black sponge” appearance is observed on T2-weighted images. This appearance is due to the stromal components the fibrous septa which often have low signal while the cystic components can have high signal; giving a “black sponge” like appearance.
Recent Comments