
Case contribution: Dr Radhiana Hassan
Clinical:
- A 70 years old man
- Chronic active smoker
- Presented with chronic cough for 3 months
- Associated with loss of weight about 10 kg
- No other symptoms
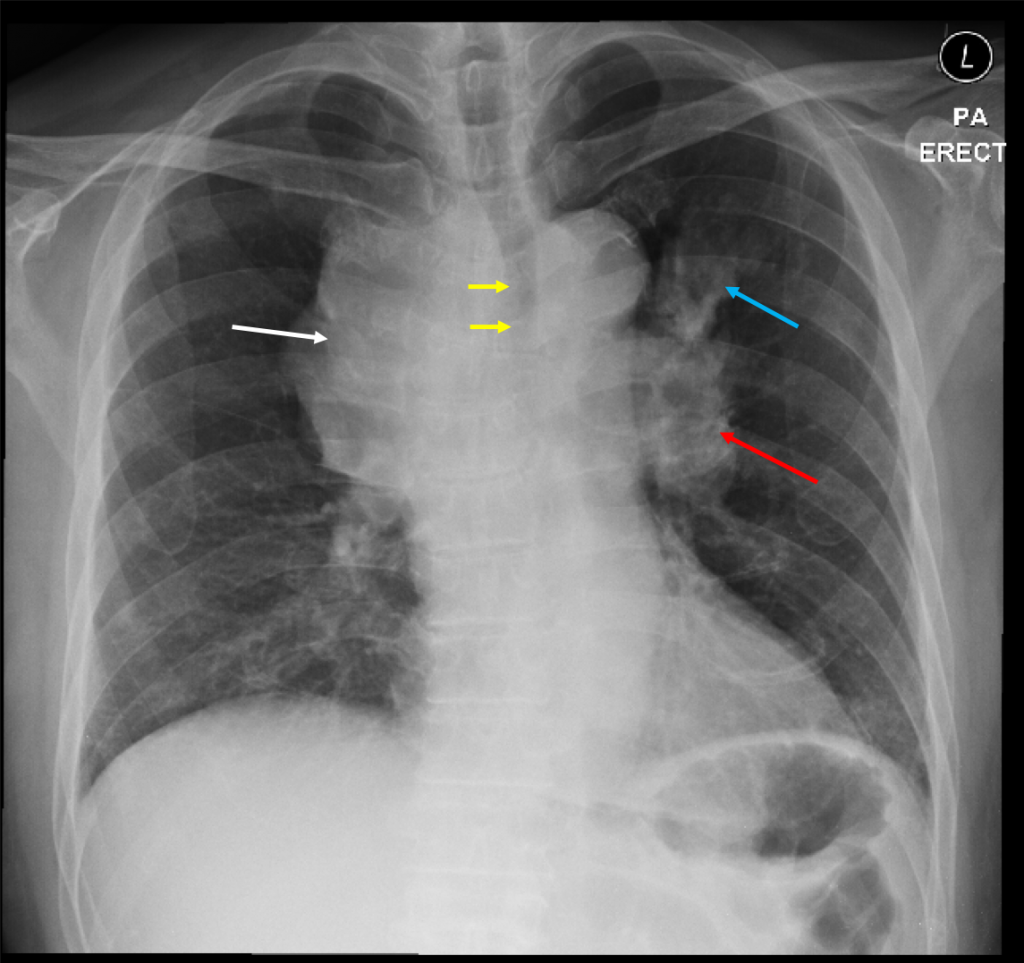
Radiographic findings:
- There is mediastinal widening with lobulated outline of mediastinal contour on the right side (white arrow).
- Compression with displacement of the trachea to the left side (yellow arrows). Minimal luminal narrowing of the trachea is seen at this level.
- There is lobulated left hilar outline (red arrow).
- An ill-defined lesion is seen the left upper zone (blue arrow). No obvious cavitation or calcification within the lesion is seen.
- No pleural effusion or pneumothorax. Bones are unremarkable.
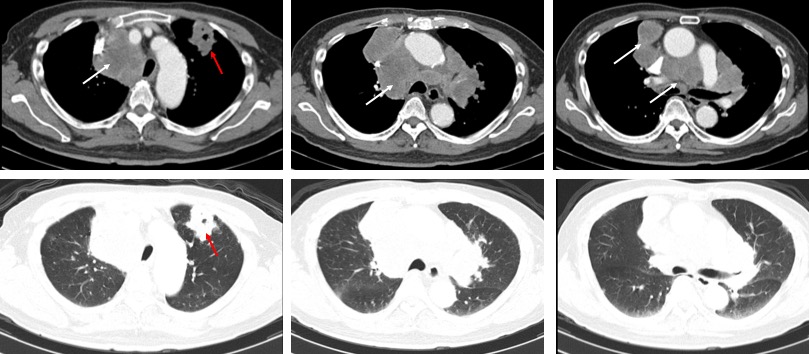
CT scan findings:
- There are multiple enlarged mediastinal nodes (white arrows). Some of the nodes are matted and non measurable.
- The enlarged nodes is causing compression and displacement of the superior vena cava.
- There is compression, distortion and minimal narrowing of the upper trachea.
- The largest node is seen at right upper paratracheal node measured 59 mm.
- There is a lobulated lesion in the anterior segment of the left upper lobe (red arrows). The lesion measures 40 mm with intralesional cavities. No calcification within it. Some speculations are seen surrounding the lesion.
- There are multiple small nodules with generalised distributions in both lung fields.
- No pleural effusion or pleural thickening. No pneumothorax.

HPE findings:
- Macroscopy: specimen labelled as lung biopsy consist of whitish tissues
- Microscopy: sections show strips of fibrocollagenous tissue infiltrated by malignant tumour arranges as cord and sheets. The tumour is associated with a lot of tumour necrosis. The tumour cells are moderately pleomorphic, having vesicular to hyperchromatic nuclei and some have prominent nucleoli. The nuclei are eccentric. The cytoplasm is moderate in amount and vacuolated. Abnormal mitotic figure is identified. There is no glandular or squamous differentiation noted.
- Immunochemical staining: CK7, CK20 are positive. TTF-1 and P-40 are negative. Special stain PAS is positive.
Diagnosis: Lung adenocarcinoma with mediastinal lymphadenopathies and distant metastatic foci.
Discussion:
- Identification of the metastatic lymph node is extremely critical in lung carcinoma.
- ON CT scans, lymph nodes larger than 1.0 cm were considered as enlarged nodes.
- There is no change made for 8th edition TNM staging of the lymph nodes
- N1-nodes are ipsilateral nodes within the lung up to hilar nodes. Presence of N1-nodes alters the prognosis but not the management.
- N2-nodes represent ipsilateral mediastinal or subcarinal lymphadenopathy.
- N3-nodes represent contralateral mediastinal or contralateral hilar lymphadenopathy or scalene or supraclavicular nodes. These are irresectable.
Recent Comments