
Case contribution: Dr Radhiana Hassan
Clinical:
- A 59-year-old man with underlying hypertension for many years
- Presented with generalized body weakness and one episode of altered behaviour.
- He was referred from another hospital for further management of pituitary apoplexy.

MRI findings:
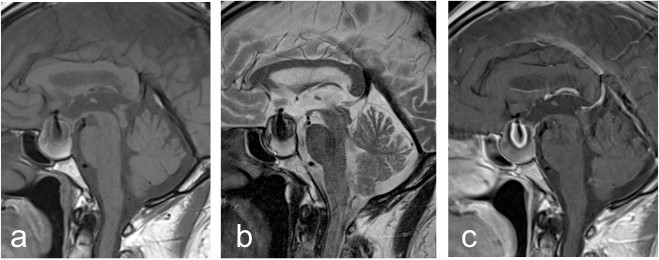
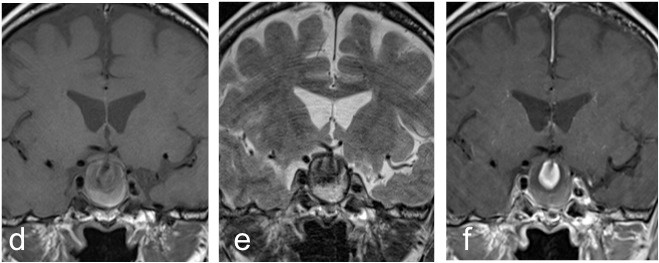
- MRI brain in sagittal (a) T1-weighted, (b) T2-weighted and (c) T1 post gadolinium and coronal (d) T1-weighted, (e) T2-weighted and (f) T1 post gadolinium
- It shows an intrasellar lesion. This lesion is rounded, well-defined and showed laminated appearance with heterogenous high signal intensity peripherally on T1 and T2-weighted images with central hypointensity.
- It also showed central enhancement post contrast.
- A 3-D reformatted MRA image revealed a saccular aneurysm arising from the anterior communicating artery (ACOM) directed antero-inferiorly (arrow).
Diagnosis: Partially thrombosed intrasellar aneurysm.
Discussion:
- Aneurysm with intrasellar extension is not common and often masquerade as pituitary tumours.
- It may potentially lead to a catastrophic outcome if they are not appropriately recognized before surgical intervention.
- The average patient age was 57 years with females accounting for 68% of the cases.
- The most common artery of origin for intrasellar aneurysm was the Internal carotid artery (ICA) which give rise to 90% of reported aneurysm while the remaining 10% from the anterior communicating artery (ACOM).
- The intrasellar ICA aneurysm often arise from the cavernous or clinoidal segment of ICA and extend into the sella turcica through the thin medial wall of cavernous sinus. Whereas the ACOM aneurysm grow inferomedially from above the diaphragm sellae.
- A minority of intrasellar aneurysm (15%) were reported to present with acute aneurysm rupture. Of all reported intrasellar aneurysms 20% presented in conjunction with coexistent pituitary adenoma.
- The rest of the cases came to clinical attention due to mass effect on surrounding structures and mostly presented with visual field defect, headache and endocrinopathy. The most commonly detected endocrinopathies were hyperprolactinemia (90%), gonadotropin deficiency (82%), ACTH deficiency (70%) and TSH deficiency (60%).
- When compared with nonfunctioning pituitary macroadenomas, intrasellar aneurysm result in comparable dysfuntion in pituitary hormone production.
- Supradiaphragmatic aneurysm are likely to be preferentially treated via surgical clipping compared to infradiaphragmatic aneurysm (ICA aneurysm) that are usually best treated with endovascular technique.
Acknowledgement:
- Prof. Ahmad Sobri Muda
- Assoc. Prof. Dr Shahizon Azura Mohamad Mukari
References/ Suggested reading:
- Cerebral aneurysms with intrasellar extension: a systematic review of clinical, anatomical and treatment characteristics. Hanak BW et al. Journal of Neurosurgery, 2012: 116(1): 164-178.
- Anterior communicating artery aneurysm in the sella turcica: a case report. Murai Y et al. Surg Neurol 2004; 62(1): 69-71
Recent Comments