
Case contribution: Dr Radhiana Hassan
Clinical:
- A 25 years old man
- Involved in MVA, motorbike skidded
- Noted to have multiple abrasion wounds at abdomen
- CXR revealed a fracture of left posterior 10th rib
- Patient was discharged home
- A few hours later fainted at home. Prior to that complaint of abdominal pain and shortness of breath
- In ED, noted to be pale. Hb drop from initial reading of 12.7 gm/dL to to 9.6 gm/dL
- BP=108/62mmHg and PR=86bpm
CT scan findings:
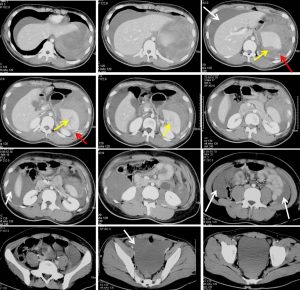
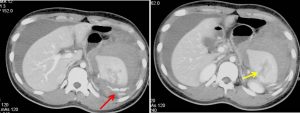
- Multiple lacerations within the spleen (yellow arrows) more than 3 cm in parenchymal depth, no involvement of the hilum with normal homogenous enhancement of the spleen.
- There is contrast extravasation (red arrows) suggestive of active hemorrhage.
- Massive hemoperitoneum (white arrows) also noted with blood pooling at perihepatic, perisplenic, both paracolic gutter and pelvis.
- Sentinel clot sign seen with higher density of hemoperitoneum at perisplenic region suggestive the site of bleed.
- No other organ injuries.
- Non-displaced left 10th rib fracture on the left side (image not shown)
Intraoperative findings:
- Patient developed hypovolaemic shock on table, BP drop to 40/20 mmHg
- Active resuscitation done
- Massive hemoperitoneum, blood loss of 3L.
- Splenic injury with lacerations approaching hilar region
- Liver, pancreas, stomach and bowels
- Splenectomy done
Discussion:
- Spleen injuries were reported in 30-49% of all visceral injuries in blunt abdominal trauma.
- Associated injuries include: left lobe of liver, left hemidiaphragm, left adrenal gland and pancreatic tail
- Grade III injury defined as lacerations more than 3 cm or intraparenchymal haematoma less than 5 cm. Presence of >50% surface area subcapsular haematoma or ruptured subcapsular haematoma also included in this grade.
- In hemodynamically stable patients, most splenic injuries are treated non-operatively. However, in haemodynamically unstable patients, practice varies from institution to institution and case to case basis.
Recent Comments