
Case contribution: Dr Radhiana Hassan
Clinical:
- A 20 years old male
- No known medical illness
- Presented with left eye blindness and ptosis
- No headache, no fever no constitutional symptom
MRI findings:
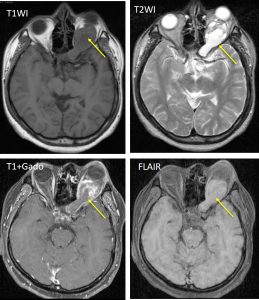
- There is left proptosis.
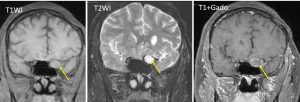
- A heterogenous mass with solid and cystic component is seen in the intraconal region of the left orbit (yellow arrows).
- There is enhancement of the solid component post contrast and rim enhancement of the cystic component.
- This mass extends posteriorly, enlarging the left optic foramen.
- No involvement of optic chiasm.
- The recti muscles are in close proximity to the mass.
- The right orbit and contents are normal.
Diagnosis: Optic nerve glioma (HPE proven)
Discussion:
- Optic nerve glioma is part of optic pathway glioma
- They are the most common primary neoplasm of the optic nerve
- Histologically these tumours are pilocytic astrocytomas
- Typically present in children, adult forms are rare and usually aggressive
- CT is often the first investigation performed and although not as sensitive as MRI.
- The optic nerve is variably enlarged, and the mass may either be fusiform or exophytic in appearance. Additionally, the nerve may be elongated with kinking or buckling 5.
- MR imaging is optimal for showing the relationship of the mass to the hypothalamus, optic chiasm, and infundibulum as well as the intraorbital and intercanalicular components of the mass.
- Large tumors are typically heterogeneous with cystic and solid components.
- T1 – enlargement, often iso to hypointense compared to the contralateral side
- T2 – hyperintense centrally, thin low-signal at the periphery representing the dura
- T1 C+ (Gd) – enhancement is variable
Recent Comments