
Case contribution: Dr Radhiana Hassan
Clinical:
- A 66 years old lady
- History of colicky abdominal pain for 2 years
- More at right hypochondriac region
- No constitutional symptom
- No fever, no vomiting, no jaundice
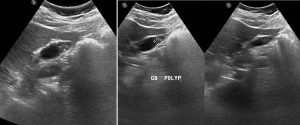
Ultrasound findings:
- Gallbladder is partially distended. The wall is normal and intact.
- No pericholecystic fluid seen. No stone seen within it.
- A soft tissue polyp measuring 1.0x 0.8 cm size at fundal area. No distal shadowing or enhancement.
- Liver is normal in size and shows homogeneously raised echotexture. No focal mass or cyst seen. No intrahepatic biliary dilatation.
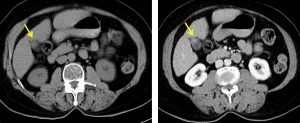
CT scan findings:
- Gall bladder is partially distended.
- There is an enhancing lesion is seen in the fundus of gall bladder measuring about 1.2 x 1.1cm.
- No calculus is seen within.
- Gall bladder wall is not thickened and no pericholecystic collection seen.
Intra-operative findings:
- Laparascopic cholecystectomy done
- Adhesion at gall bladder bed
- Cirrhotic liver
- Polyp at fundus of gall bladder 2×2 cm
HPE findings:
- Macroscopy: specimen labelled as gallbladder consist of a surgically cut open gall bladder measuring 65x30x12 mm. There is no stone within the lumen. On further sectioning revealed a nodule at the fundus measuring 30x25x5 mm with grayish white cut surface containing multiple cystic spaces. The wall of the gallbladder measures 4 mm in thickness. No malignancy seen.
- Microscopy: sections from nodule at fundus shows proliferation of the mucosal glandular structures inceptiving from the mucosa of gallbladder with hyperplasia of the smooth muscle cells. Aggregation of cystically dilated glandular structures are surrounded by a hyperplasic smooth muscle tissues and are lined by uniform columnar epithelium. No nuclear atypia seen. The remaining gallbladder wall sows areas of denuded epithelium with mild lymphoplasmacytic cells infiltrate. Scattered Rokitansky-Aschoff sinuses are present. The muscular layer are hypertrophied. The serosa is unremarkable. No dysplasia or evidence of malignancy seen.
- Impression: Gallbladder adenomyomatous hyperplasia with chronic cholecystitis
Diagnosis: Gallbladder polyp (benign)
Discussion:
- Gallbladder polyps are frequently detected with increased used of imaging.
- Majority of polyps are non-neoplastic and represent cholesterol or inflammatory polyps
- For neoplastic polyp, malignant transformation to adenocarcinoma is a primary concern
- The suggested follow up of gallbladder polyps
- –No further follow up if lesion ≤ 6 mm
- Follow up 3-6 months for lesion 6-9 mm
- Surgical consultation if lesion ≥ 10 mm
- Risk of malignancy increased in polyps ≥ 10mm (most well established risk factor), sessile polyps, single polyps, polyps with adjacent wall thickening, invasion of wall and older age group.
- Adenomyomatous hyperplasia of the gall bladder is also known as adenomyomatosis or diverticular disease of gallbladder. It is benign and usually asymptomatic and relatively common in cholecystectomy specimens . About 80% are associated with chronic cholecystitis. It is rarely associated with dysplasia and carcinoma.
Recent Comments