
Case contribution: Dr. Radhiana Hassan
Clinical:
- A 64 years old man
- No underlying medical illness
- Start to have blurring of vision for one month
- Initially presented with left sided body weakness, x-ray, ECG and blood investigation done in a district hospital were normal. Patient was discharged home.
- After that had worsening of limb weakness and unable to talk and not obeying command
- CT scan done at a private center shows a mass in the brain
- Referred for further management
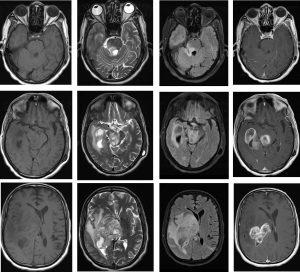
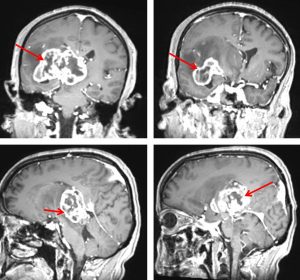
MRI findings:
- There is a huge lobulated mass with the epicentre seen at the right thalamus (red arrows) measuring about 6.2 cm x 6.6 cm x 4.2 cm (AP X W X CC).
- There is significant associated perilesional oedema
- The mass appears hypointense with peripheral hyperintense on T1, heterogeneous mixed hypo and hyperintense on T2/FLAIR and vividly enhancing post contrast.
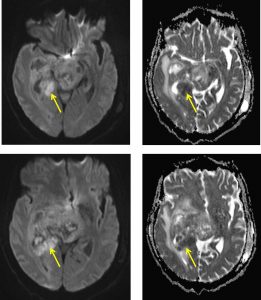
- Areas of restricted on DWI/ADC at the periphery of the mass lesion (yellow arrows).
- Multiple areas of cystic/ necrotic area within the mass.Blooming artifacts also seen on GRE (images not shown).
- The mass is seen extending to the right midbrain, right pons and right cerebellar peduncle.
- There is midline shift to the left measuring about 1.4 cm.
HPE findings:
- Macroscopy: specimen labelled as brain tissues.
- Microscopy: section shows fragments of tumour tissue, composed of sheets of cellular neoplastic cells in a fibrillary background. The neoplastic cells exhibit moderate to markedly pleomorphic nuclei, hyperchromatic nuclei with occasional small prominent nucleoli and scanty cytoplasm. Mitotic figures are present including abnormal form. Scattered multinucleated tumour are also seen. In areas, pseudopalisading necrosis and focal microvascular proliferations are noted.
- Immunohistochemistry, the neoplastic cells are GFAP positive and Ki67 proliferative index 15%.
- Interpretation: Glioblastoma WHO Grade IV
Diagnosis: Glioblastoma multiforme
Discussion:
- Glioblastoma multiforme is a grade IV astrocytoma aka malignant astrocytoma
- It can occur at any age but peak at 45-75 years old.
- There is male predominance.
- Most common seen in supratentorial white matter> brainstem> cerebellum
- On CT scan it is seen as irregular isodense or hypodense mass with central hypodensity representing necrosis. Marked mass effect and surrounding oedema is seen. Hemorrhage is not uncommon. Calcification is rare. Strong heterogenous enhancement on post contrast.
- T1WI shows isointense or hypointense irregular mass and may contain subacute hemorrhage.
- T2WI shows heterogenous hyperintense mass with adjacent vasogenic oedema. Necrosis, cyst, hemorrhage and flow voids due to neovascularity may be seen.
- FLAIR shows heterogenous hyperintense mass iwth adjacent vasogenic oedema.
- DWI typically shows no restricted diffusion.
- Post contrast shows thick irregular rind of enhancement surrounding central necrosis.
- MRS shows decreased NAA and myoinositol. Elevated choline, lactate and lipid peak.
- PET scan shows high glucose metabolism and avidly accumulate FDG.
- Prognosis is poor (death in 9-12 months)
Progress of patient:
- Decided not for further treatment
- Defaulted follow up.
Recent Comments