
Case contribution: Dr Radhiana Hassan
Clinical:
- A 36 years old lady
- Presented with bilateral upper and lower limb weakness 3 years ago
- Noted worsening of the weakness. Currently requiring wheelchair to ambulate
- Refused lumbar puncture
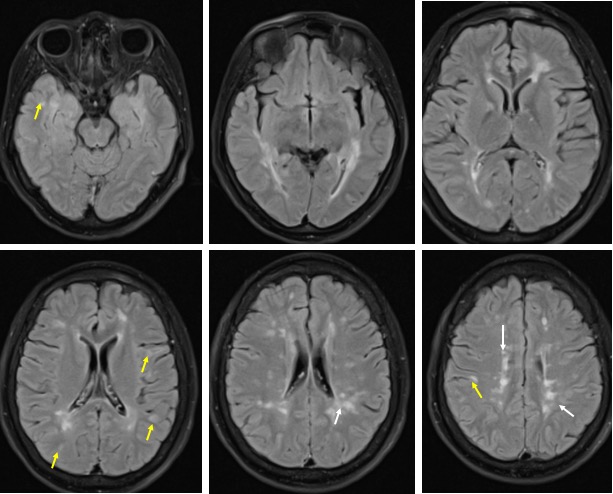

MRI brain findings:
- Multiple hyperintense lesions are seen in FLAIR and T2 sequences.
- These are mainly present in both periventricular regions (white arrows) of both frontal, parietal and occipital lobes, with their long axis directed perpendicular to the lateral ventricles. They range in size, with the largest seen in the left cerebral hemisphere, measuring 13 mm in maximal diameter.
- Bilateral cortical, juxta-cortical (yellow arrows) and white matter lesions are also seen, although these are less in number compared to the peri-ventricular lesions. These are seen towards the vertex in the parietal lobes and in the temporal lobes.
- Other lesions are seen in both basal ganglia.
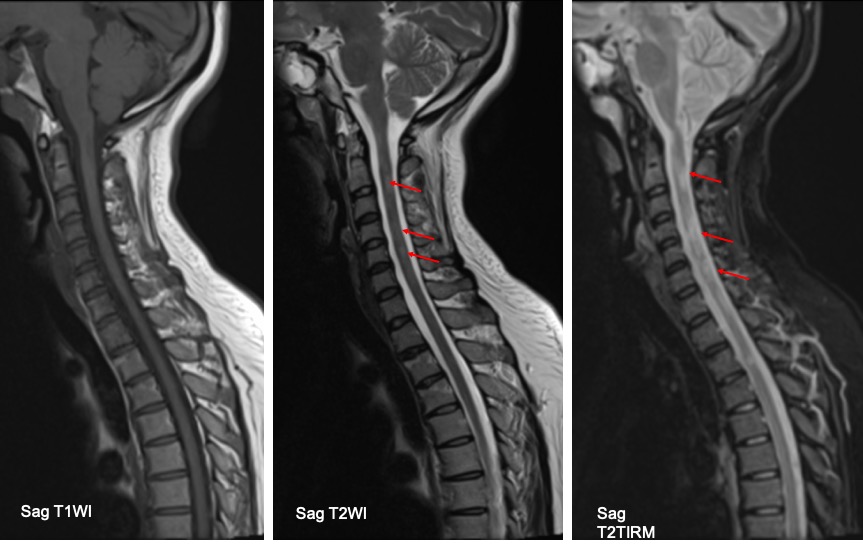
MRI of spine:
- There are patchy T2/TIRM hyperintense lesions involving mainly the cervical spine
- Less severe involvement is seen at thoracic region
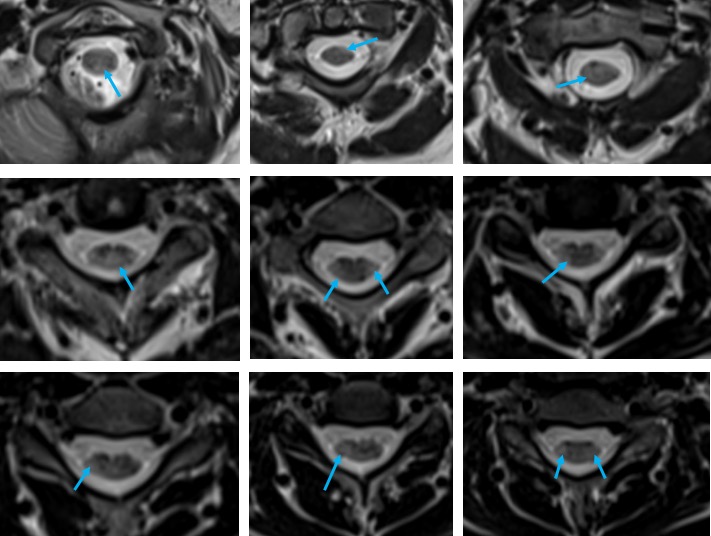
- On axial cut these patchy hyperintense lesions are located at posterolateral, lateral and few are also involving anterolateral region
- No expansion of cord
- No enhancement of any of the lesions
Diagnosis: Multiple sclerosis
Discussion:
- Multiple sclerosis is a chronic relapsing demyelinating disease
- It is the second most common cause of neurological impairment in young adult after trauma
- Peak incidence is at about 35 years of age
- MRI is so far the most sensitive technique for detecting multiple sclerosis (MS) lesions and has proved to be an important paraclinical tool for diagnosing MS and monitoring therapeutic trials
- MS lesion plaques have a predilection for periventricular white matter and tend to have an ovoid configuration with the major axes perpendicular to the ventricular surface.
- In addition to the periventricular region, other regions frequently involved are the corpus callosum, subcortical region, brain stem, U-fibers, optic nerves, and visual pathway
- The focal demyelinating lesions located along the lateral borders of the corpus callosum are best depicted by sagittal fluid-attenuated inversion recovery (FLAIR) imaging
- Optic neuritis, which appears early and may be the only presentation in the initial stage of MS, can be detected by using a fat-suppression technique combined with contrast-enhanced imaging or by using long-echo short-tau inversion recovery (STIR) imaging
Recent Comments