
Case contribution: Dr Radhiana Hassan
Clinical:
- A 39 years old man
- Alleged MVA
- Complaint of pain at epigastric region
- BP=110/80 mmHg, PR=80 bpm, GCS=15/15
CT scan findings:
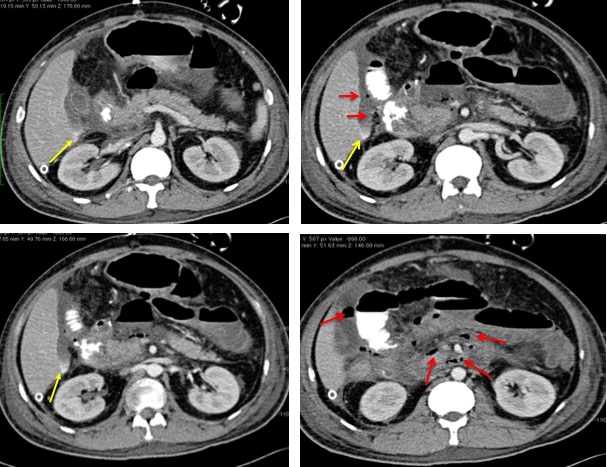
- Multiple air pockets at duodenal region (red arrows)
- Presence of contrast extravastion at inferior perihepatic region (yellow arrows)
- Suspicious wall thickening and irregularity at D3 region
- Associated massive hemoperitoneum
- No solid organ injury
Intra-operative findings:
- Transected second part of duodenum, about 90% circumferential transection
- Pancreatic body injury
- Also had multiple serosal tear at colon
- Estimated blood loss 2.5 L
- No solid organ injury
- close proximal and distal end anastomosis of transected duodenum
- Roux-en-Y pylorojejunostomy anastomosis with lesser curvature
- jejuno-jejunostomy
- repair of serosal tear of colon done
Diagnosis: Blunt abdominal trauma with bowel injury (transected duodenum)
Discussion:
- Injuries of the duodenum in blunt abdominal trauma are uncommon due to its retroperitoneal location
- Early diagnosis is critical and the time interval from injury to definite treatment influences morbidity and mortality from this injury.
- CT scan is the imaging modality of choice for assessment of patients but it cannot always distinguish duodenal perforations from duodenal haematomas. In this case suspicious perforation is because of contrast extravasation and presence of free air.
- A combined injury of the pancreas and duodenum has been regarded as a separate category of injury, with a particularly high mortality
Recent Comments