
Case contribution: Dr Radhiana Hassan
Clinical:
- A 43 years old man
- IVDU, Hep C +ve, PTB +ve (completed treatment 9 years ago)
- Alleged assaulted in Pusat Serenti
- Complaint of abdominal pain
- Clinically tender and guarded abdomen. BP=164/93mmHg, PR=75 bpm and GCS=15/15
- Multiple laceration wound at scalp region. Skull radiograph shows no fracture.
- Abdominal radiograph shows no pneumoperitoneum.
- Ultrasound shows bilateral hydronephrosis with free fluid at perisplenic region
CT scan findings:
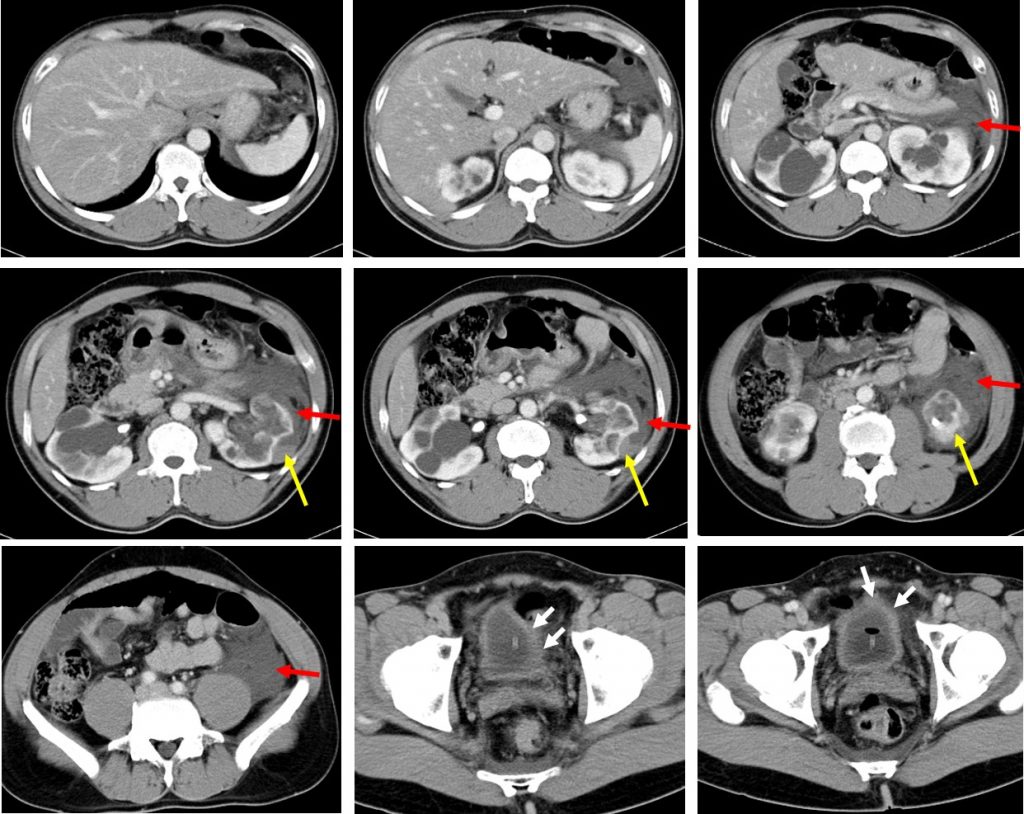
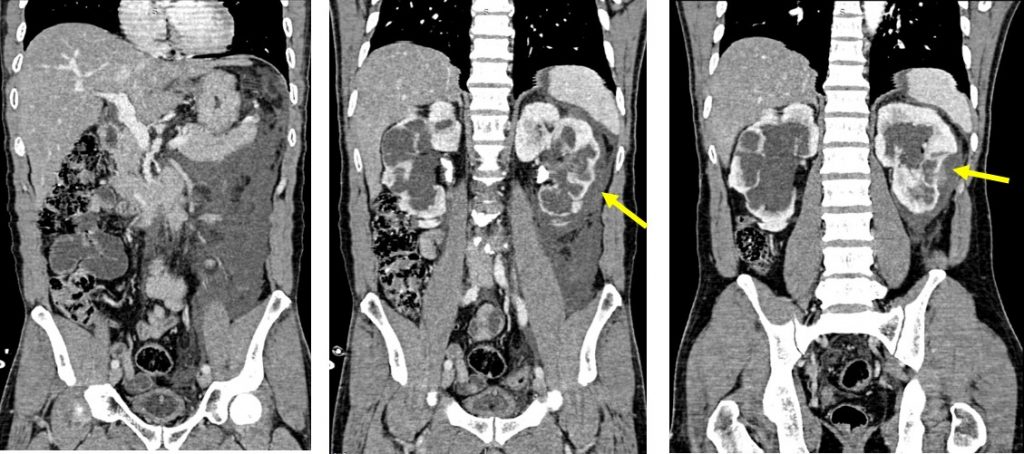
- There is a small laceration at lower pole of left kidney with surrounding perinephric hematoma (yellow arrows). Blood collection is seen tracking inferiorly (red arrows).
- The laceration is not extending to collection system.
- No other organ injury is seen.
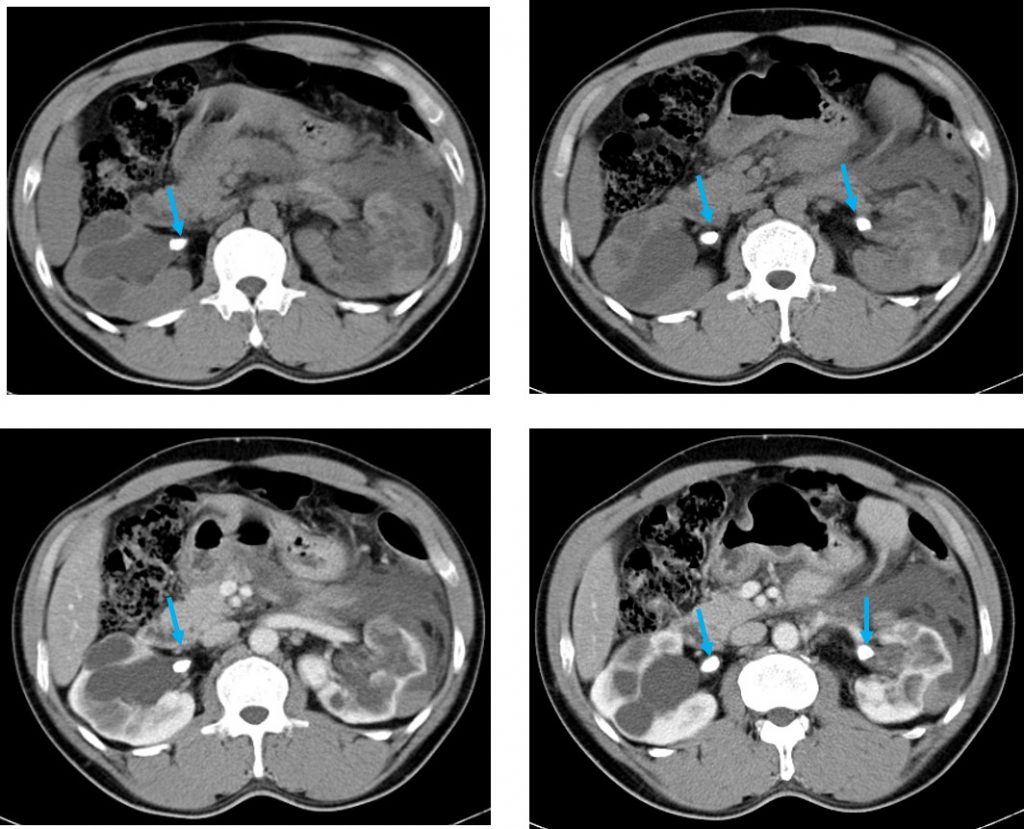
- There is bilateral moderate to severe hydronephrosis. Presence of calculi at both renal pelvis (blue arrows)
- Urinary bladder is underfilled with suspicious wall thickening at left side.
- Prostate is not enlarged.
Progress of patient:
- Bilateral RPG shows bilateral moderate to gross hydronephrosis
- No hydroureter seen
- Filling defect is seen at both PUJ in keeping with calculi
- Failed to stent right side, left ureteric stenting was successful
- Bladder growth is seen at trigone region. Biopsy taken.
HPE findings:
- Polypoidal tissue covered by 6-7 layers of urothelial cells.
- The lamina propria show a dense inflammatory cells infiltrate rich in eosinophils
- Fibrosis and few multinucleated giant cells are seen in lamina propria.
- No malignancy seen.
- Interpretation: Eosinophilic cystitis
Diagnosis: Grade II renal injury with underlying eosinophilic cystitis
Discussion:
- Eosinophilic cystitis is a rare urological disease simulating bladder tumour.
- The incidence is uncertain and it affects patient of all ages.
- The etiology of eosinophilic cystitis remains unclear.
- It is characterized by inflammation, mainly by eosinophils throughout all layers of the bladder wall and fibrosis of the mucusa and muscularis necrosis.
- The typical manifestations are irritative bladder symptoms and most common cases with large bladder mass simulating bladder carcinoma.
- Ultrasound and CT scan show diffuse or irregular bladder wall thickening which may be seen as tumour-like lesion. Bilateral upper tract dilatation is seen of different severity. Urography revealed small contracted bladder and hydronephrosis.
- Because of the rareness of this disease, standardized therapy regimen do not exist.
- Based on changes in differential reaction to corticosteroid and/or antihistamin, patients were divided into 3 groups
- Group 1: asymptomatic and no need treatment
- Group 2: good response and cured by oral corticosteroid and/or antihistamin
- Group 3: deterioration of symptoms although intense medicine therapy and need surgery
Recent Comments