
Case contribution: Dr Radhiana Hassan
Clinical:
- A 13 years old boy
- Had underlying Brugada syndrome on pacemaker and T.propanolol ,under IJN follow up
- Presented with left hip pain for 5 days
- Sudden onset, no swelling, ho history of trauma
- Also had fever with URTI symptoms
- Clinically not septic looking, left hip in flex position, tender on palpation, warm but not erythematous. Limited range of motion of hip joint due to pain. Left knee is normal.
- Renal function test normal, Hb=12.8 g/dL, TWBC=11.8/L

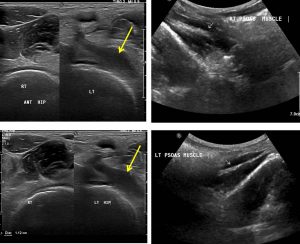
Ultrasound findings:
- The iliopsoas muscles se are symmetrical and normal. No collection seen in it.
- Both hip joints scanned anteriorly and comparison made in corresponding areas.
- There is deep intra muscular collection, just anterior to hip joint pain and tracts inferiorly.
- It is hypoechoic with internal echoes within it. It measured about 5cm x 1.1 cm in dimension.
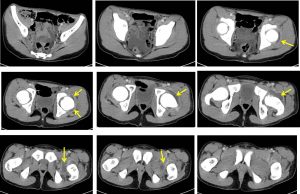
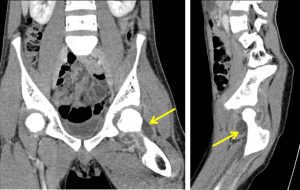
CT scan findings:
- There is effusion in the left hip joint; HU ranges from 9-15 with wall enhancement on post contrast images (yellow arrows).
- The surrounding muscles are seen minimally pushed and compressed. However, there is no obvious involvement of the adjacent muscles.
- The iliopsoas muscles on both sides are normal.
- No lytic or sclerotic changes of the femoral head and the acetabulum (bone window images not shown).
Progress of patient:
- Left hip arthrotomy and washout done
- Pus at left hip about 10 cc
- C&S result, no growth
- Gram stain shows gram positive cocci
- Tissue C&S: strep group A, AFB not seen
- Completed 2 weeks of IV antibiotics and discharged well
Diagnosis: Septic arthritis of left hip
Discussion:
- Septic arthritis is a common, often disabling disease that requires early diagnosis for optimal outcome.
- The most commonly affected joints are large joints with abundant blood supply such as shoulder, hip and knee.
- Early diagnosis is important to avoid complications such as cartilage and joint destruction, osteonecrosis, secondary osteoarthritis, osteomyelitis, and eventually ankylosis.
- Effusions have been considered a sine qua non of septic arthritis and present in 75% of cases.
- Thickening and abnormal enhancement of the synovium is other findings of septic arthritis.
- Synovial enhancement and joint effusions had the highest correlation with the clinical diagnosis of septic joint.
- MRI have higher sensitivity to detect coexistent osteomyelitis in patients with septic arthritis
- Brugada syndrome is abnormal ECG in structurally normal heart with high incidence of sudden death in young patient.
Recent Comments