
Case contribution: Dr Radhiana Hassan
Clinical:
- An 11 months old baby
- Picked up 10 cent coin and swallowed
- Witnessed by mother
- Post ingestion, child cried and vomiting once, milk content vomitus
- No rapid breathing, no noisy breathing
- Clinical examination is unremarkable
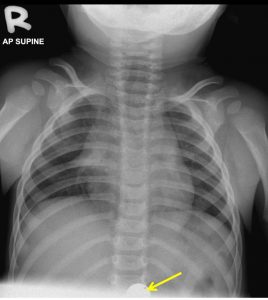
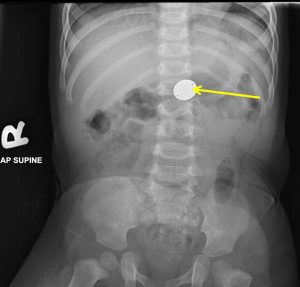
Chest and abdominal radiograph findings:
- The radiographs show a rounded metallic foreign body overlying the stomach region in keeping with coin as described by mother (yellow arrow)
- No evidence of intestinal obstruction
- No pneumoperitoneum to suggest bowel perforation
- Lungs are clear and normal
- Thymus shadow is seen, normal at this age group
Diagnosis: Coin ingestion with no obvious complication seen.
Progress of patient:
- Patient was discharged home
- Advice to parent to come back if coin not passed within 2 weeks
- Symptoms of intestinal obstruction also explained and to come again immediately if patient is symptomatic.
- Patient was well after that, presented again 8 months later with another episode of swallowing foreign body
Discussion:
- Coins are the most commonly swallowed foreign body that comes for medical attention in children.
- Most of the ingestion are accidental and children with psychological impairment are at high risk for foreign body ingestion.
- Most of the time the swallowed coin will harmless pass through the GI tract.
- The most common site for obstruction is at thoracic inlet, which is area between the clavicles on chest x-ray. Another common site of obstruction is in the mid-esophagus at the level of carina and aortic arch. Lower esophagus at esophageal junction is another site of entrappment.
- Large object >6cm long and >2cm wide may become entrapped at pylorus
- High risk for complications of coin ingestion include children with pre-existing gastro-intestinal tract abnormalities such as congenital malformations, neuromuscular disease and eosinophilic esophagitis.
- X-rays covering the esophagus to beyond pylorus can be done for assessment. If no coin seen or coin seen in stomach or beyond and child looks well, pain-free, no respiratory distress and able to eat or drink, the child can be discharge with advice.
- Parent may be advised to inspect the stool for foreign body to pass out. Radiographic follow up once a week is sufficient unless patient is symptomatic.
- Consider referral if child is symptomatic, the coin is seen lodged in esophagus and child has significant past medical history.
Recent Comments