
Case contribution: Dr Radhiana Hassan
Clinical:
- A 55 years old man
- No known medical illness, chronic smoker
- Presented with vomiting for the past 10 days
- History of progressive dysphagia for the last few weeks
- Associated with significant weight loss
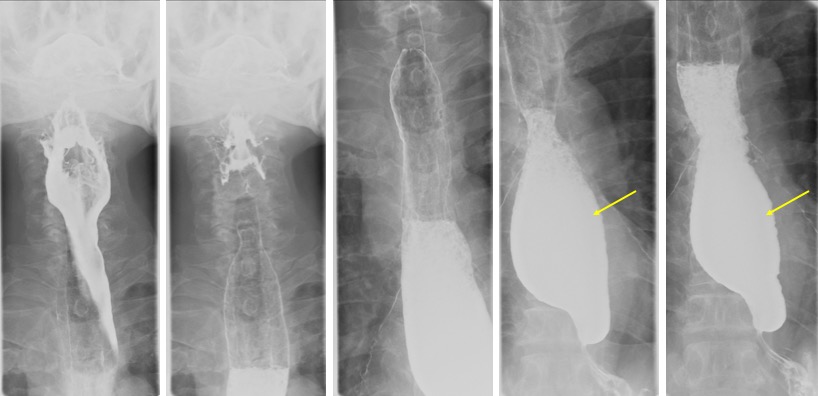
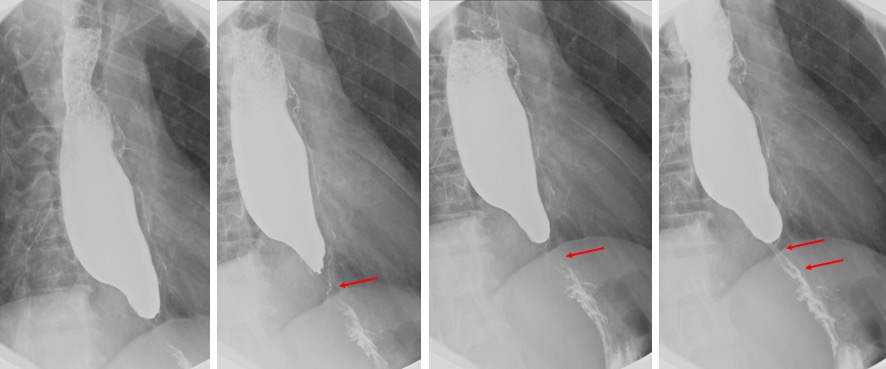
Barium swallow findings:
- Upper esophagus is normal
- The lower third esophagus is dilated.
- Pooling of contrast and food residue seen within this dilated portion of esophagus.
- Abrupt narrowing of the distal esophagus.
- No obvious irregularity at its wall.
- No obvious filling defect or mucosal abnormality seen.
- Minimal intermittent trickling of contrast into the stomach is seen.
Progress of patient:
- OGDS shows esophageal stricture. Unable to pass scope beyond 40 cm. No mucosal abnormality
- CT scan shows soft tissue mass within the distal esophagus causing narrowing of the lumen. The mass has infiltrated the lower esophageal wall anteriorly. There is indentation of thoracic aorta.Proximal esophagus is dilated. Multiple mediastinal node enlargement. Soft tissue mass at posterior chest wall with adjacent rib erosion.
Diagnosis: Esophageal stricture secondary to neoplasm (esophageal carcinoma)
Discussion:
- An esophageal stricture is a narrowing of the lumen due to inflammation or tumour.
- It may be localized or diffuse and may have abrupt or tapered margins.
- Benign strictures usually show smooth tapering and concentric narrowing. Malignant strictures are manifested by irregular narrowing and constriction of the lumen with ulcerated and nodular mucosa, abrupt well-defined proximal and distal borders.
- SCC tend to involve upper esophagus and adenocarcinoma are located in distal third.
Recent Comments