
Case contribution: Dr Radhiana Hassan
Clinical:
- A 33 years old man
- Non-smoker and no known medical illness
- Presented with anterior neck swelling for 2 months
- Associated with odynophagia, dysphagia, exertional dyspnoe and loss of weight (about 9 kg in one month)
- No fever, no night sweat, no PTB contact
- Father died of lung cancer
- Clinical examination shows diffuse swelling over the anterior neck which is soft and mild tender on palpation. Facial plethora seen. No other remarkable findings. Pemberton’s sign negative
- Hb=14.9, TWBC=4.6, Plt 320, ESR normal, CRP raised.

Findings:
- There is soft tissue swellling at prevertebral region extending to involve entire cervical region (white arrows)
- No air pockets within. No radiopaque foci to suggest foreign body.
- Bones are otherwise normal in appearance.
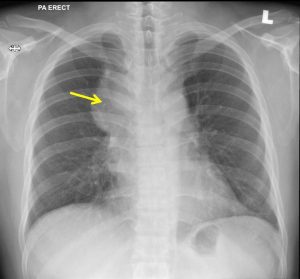
Chest radiograph findings:
- There is mediastinal widening
- No calcification or air pockets within it
- No obliteration of overlying hilum
- No extension to supraclavicular region
- No significant mass effect or displacement of trachea
- Spine is normal. Paraspinal region are also normal.
- No crowding of ribs.
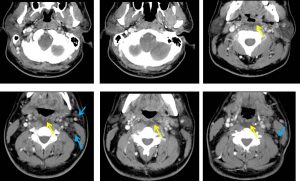
CT neck findings:
- Elongated thickened retropharyngeal is observed extending from the level of C1 until C5 vertebra (yellow arrows).
- It measures at about 1.0 x 2.7 x 8.1cm.
- It is hypodense (CT HU:15-25) with no significant enhancement.
- No calcification seen or air pockets within.
- Numerous shotty nodes are seen throughout both triangles on both sides of the neck, more apparent on the anterior triangles (blue arrows).
- Presence of right IJV thrombosis.
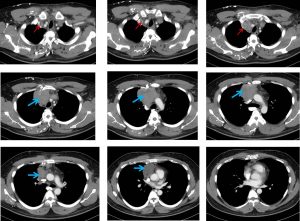
CT scan findings:
- There is anterior mediastinal soft tissue mass with evidence of extensive mediastinal lymphadenopathies
- Superior vena cava obstruction and IJV thrombosis (red arrows) with numerous collateral chest wall venous channels
- Extensive cervical nodes are also observed. Given the presence of extensive lymphadenopathies
Progress of patient:
- Rhinonasal examination shows inferior turbinate mildly hypertrophied and pale, OMC clear, symmetrical fossa of rossenmuller
- FNPLS shows posterior pharyngeal wall bulding at oropharyngeal and nasopharyngeal level, no mass, no ulceration. Pyriform fossa is clear. Epiglottis, arytenoids, aryepillotic folds are normal. Vocal cords are symmetrical and normal.
- Biopsy of mediastinal mass done
HPE findings:
- Macroscopy: specimen labelled as biopsy of mediastinal mass
- Microscopy: section shows strips of fibro-collagenous tissue diffusely infiltrated by sheets of malignant lymphoid cells. The malignant cells display moderate to marked pleomorphism, hyperchromatic to vesicular nuclei with prominent nucleoli. In areas multinucleated tumour giant cells are noted. Mitoses are easily seen. Necrosis are present.
- Immunohistochemistry, the malignant cells are positive ofr CD20, CD10 and negatives for CKAE1/AE3, CD3 with Ki 67 proliferative index of 80%.
- Interpretation: Diffuse largeB-cell lymphoma, GCB subtype
Diagnosis: Large B-cell lymphoma
Discussion:
- Lymphoma is a malignancy arising from lymphocytes or lympoblasts.
- Lymphoma accounts for about 4 % of all cancers.
- Lymphoma can present as nodal or extranodal disease. It can also present with fever, night sweat and weight loss.
- Two main type of lymphomas are Hodgkin lymphoma and non-Hodgkin lymphomas.
- CT scan is the main imaging modality in lymphoma and widely used in staging.
- Lymphoma cure rates are high.
- Prognosis depends on histological type, grade and stage of the disease.
Recent Comments