
Case contribution: Dr Radhiana Hassan
Clinical:
- A 24 years old man, involved in road traffic accident (MB versus car)
- Under alcohol influence
- No loss of consciousness and no ENT bleed
- Complaint of abdominal pain.
- Clinically BP=83/48mmHg, PR=103 bpm, GCS=15/15
- Ultrasound in ED shows hemoperitoneum
CT scan findings:
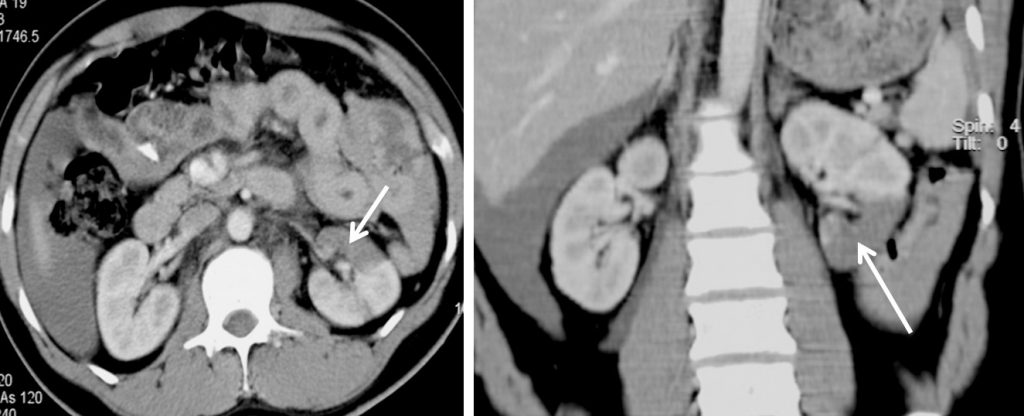
- A wedged-shaped non-enhancing hypodensity is seen at lower pole of left kidney
- No renal laceration or perinephric changes/collection
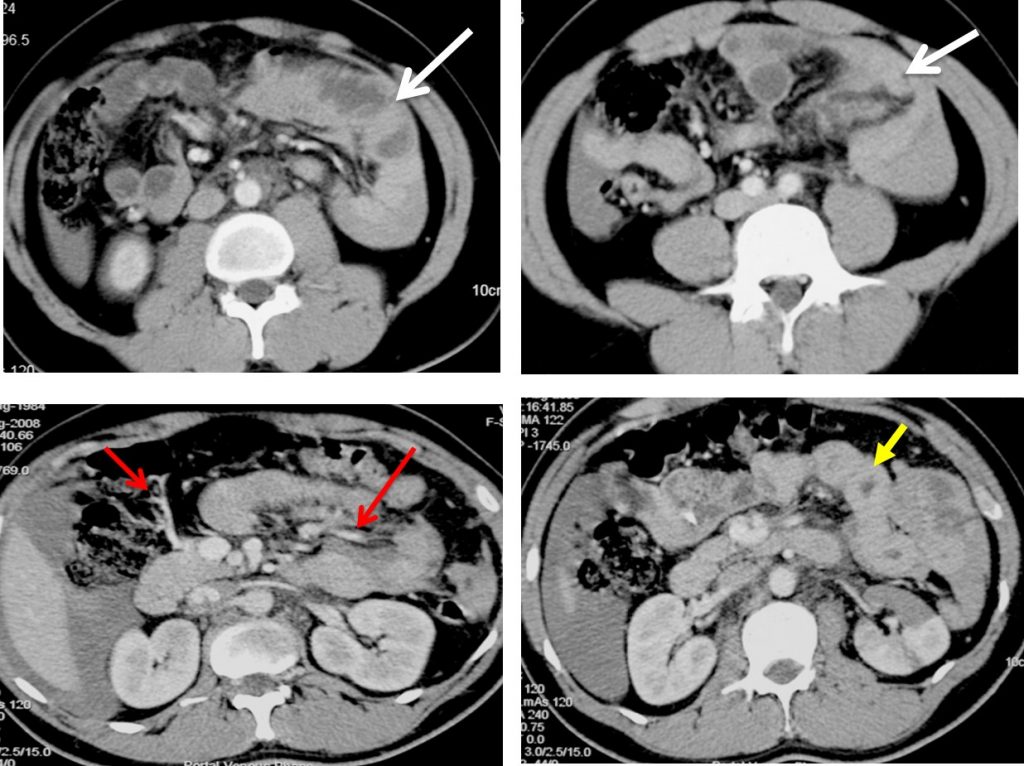
- Abnormal thickening of the small bowel wall (yellow arrow). This part of bowel loop also shows abnormal enhancement.
- Abrupt termination of mesenteric vessels opacifications are also seen (red arrows)
- Mesenteric streakiness and moderate hemoperitoneum are also seen
- No free intraperitoneal air to suggest bowel perforation
Intra-operative findings:
- Hemoperitoneum about 1L,
- mesenteric tear at multiple site with bleeding of mesenteric vessels.
- Non-viable segment of ileum due to mesenteric injury.
- Solid organs were normal.
- No retroperitoneal hematoma.
- Small bowel resection with end-to-end anastomosis done
- Patient recovered well
Diagnosis: Blunt abdominal trauma with mesenteric injury and segmental renal infarction
Discussion:
- The incidence of segmental renal infarction caused by blunt abdominal trauma is unknown.
- Renal trauma is responsible for 30.8% of acute renal infarction cases.
- Traumatic thrombosis of a segmental renal arterial branch is classified as grade 4 injury.
- Thrombosis of an intact renal artery, usually due to a shearing injury to the intima.
- Infarcts typically appear as peripherally based, wedge-shaped areas of parenchyma that
fail to enhance during both the corticomedullary and pyelographic phases of a CT study. - Segmental infarcts may be solitary or multiple and are frequently associated with other renal injuries.
- The mechanism of mesenteric injury in blunt abdominal trauma involves compression and deceleration forces which result in a wide spectrum of injuries.
- The injuries that can occur range from contusions, to tearing of the bowel wall, shearing of the mesentery and to loss of vascular supply.
- CT scan helps localise free fluids, pneumoperitoneum and mesenteric haematomas. It also helps evaluate solid organ injuries.
- CT findings of mesenteric injury include mesenteric hematoma, extravasation of intravenous contrast material, and abrupt termination and beading of vessels. Bowel wall thickening and increased bowel wall enhancement may represent bowel injury with vascular involvement.
Recent Comments