
Case contribution: Dr Radhiana Hassan
Clinical:
- A 9 years old girl, no known medical illness
- Fall from a bicycle, had bleeding and laceration at forehead
- Wound sutured and discharged home
- Mother noted bruises at the epigastric region
- Developed abdominal pain, vomiting and low grade fever
- Ultrasound done reported as no solid organ injury
- Referred for further management
- BP=100/54 mmHg, PR=102 bpm, GCS=15/15
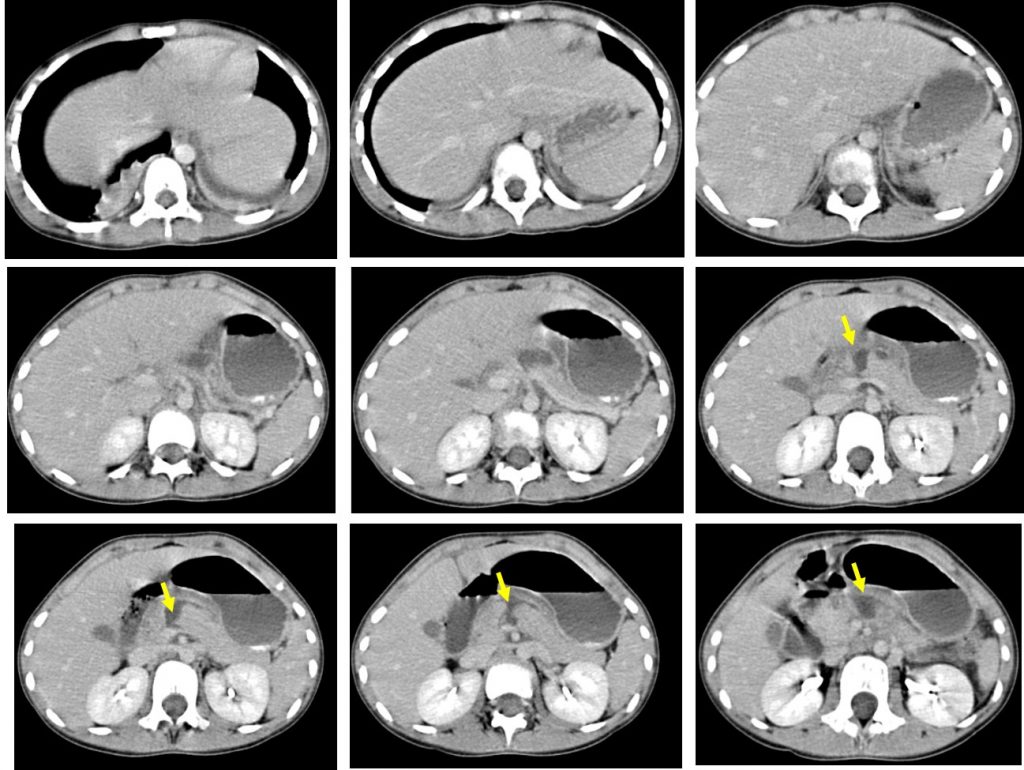
CT scan findings:
- There is a laceration at body of pancreas (yellow arrows)
- The laceration extends and involving the pancreatic duct
- Minimal peripancreatic fluid
- No other organ injury seen
Progress of patient:
- Patient was managed conservatively
- Follow up CT scan shows small pseudocyst
- Another follow up after 2 months shows larger cyst
- A percutaneous drainage was performed


Diagnosis: Post traumatic pancreatic pseudocyst
Discussion:
- Pancreatic pseudocyst occurs from disruption of pancreatic duct structure resulting in leakage and accumulation of pancreatic fluid and hemorrhagic fat necrosis.
- It is called pseudocyst as it is not lined by epithelium, but severe inflammatory reaction resulting in encapsulation of the cyst by fibrosed granulation tissue.
- On imaging it is fluid-filled structure of collection with relatively thick wall. It can be multiple and most commonly located in the pancreatic bed.
- A unilocular cyst with clinical history of trauma or pancreatitis is almost always a pseudocyst.
- It is not possibleto differentiate infected from non-infected pseudocyst on imaging alone.
- It may regress on its own with no further treatment. However, interventions are required in selected cases such as infected cyst, large size causing compression effect and symptomatic and recurring cyst.
Recent Comments