
Case contribution: Dr Radhiana Hassan
Clinical:
- A 65 years old man with underlying DM, HPT, CKD, BPH and CVA
- He was bedridden since 2 years ago but still able to do self-feeding
- Presented with fever and abdominal pain for 4 days
- Then becoming less responsive
- No URTI symptoms, no altered bowel habit
- Upon arrival at ED, BP=110/76mmHg, HR=115 bpm, RR =25 bpm, temperature=38.3 degree celcius, abdomen distended
- LFT deranged, increased TWBC (14.6 to 17.0)

Abdominal radiograph findings:
- Right renal calculus (yellow arrow)
- Prominent small bowel loops (white arrows)
- No other significant finding
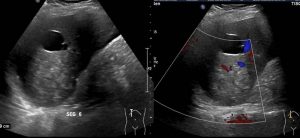
Ultrasound of abdomen findings:
- There is a round, heterogeneous lesion with fairly well-defined margin seen at liver segment VI, measuring 7.7 x 6.8 x 7.5 cm (W x AP x CC) in size. No liquefied area or calcification seen.
- A thin walled, anechoic cystic lesion is also noted adjacent to it measuring 3.3 x 2.9 x 3.1 cm. No cyst wall calcification, internal septa or soft tissue component within the cyst.
- Otherwise, rest of the liver parenchyma has normal echogenicity and smooth echotexture. No dilated biliary tree. Portal veins are normal.
- Gallbladder is well-distended. Multiple subcentimeter calculi and minimal sludge are seen within (images not shown).
- Spleen and pancreas are normal.
- Bilateral renal calculi seen (images not shown)
- Anechoic free fluid is seen at interloop, subhepatic and pelvic regions. No echogenic debris seen within the intra-abdominal free fluid.
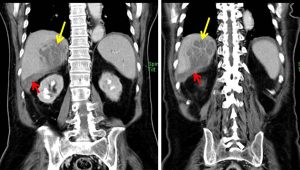
CT scan findings:
- Liver is enlarged with craniocaudal length measuring 17.1 cm.
- A lobulated hypodense lesion is seen at liver segment VI/VII (yellow arrows) abutting the liver capsule, measuring 6.9 x 7.2 x 7.0 cm (W x AP x CC). Multiple septations enhancement is seen post-contrast.
- Disruption of the adjacent liver capsule is seen at the postero-inferior part of the lesion; the capsular defect measures approximately 2.4 cm (on coronal view).
- No contrast pooling on delayed phase.
- Subhepatic, pericholecystic and right paracolic gutter collections are seen.
- Several tiny calculi are noted within the gallbladder lumen.
- Bilateral renal calculi as noted in ultrasound.
Diagnosis: Ruptured liver abscess
Discussion:
- Ruptured liver abscess is a common presenting problem of acute abdomen in developing countries
- Alcoholics, patient with diabetes and immunosuppression are at high risk for developing liver abscess.
- There is slight male preponderance and abscesses usually located at right lobe of liver.
- Unlike contained abscess where nonsurgical options can be considered, ruptured liver abscess usually needs surgical intervention.
- Percutaneous drainage via catheter, laparosocopic drainage and open surgical methods are among the choices of treatment.
- Surgical exploration with thorough peritoneal lavage improves the outcome and prognosis of the patient.
Progress of patient:
- Laparotomy and peritoneal washout done, confirmed ruptured abscess at Segment VI/VII
- Patient was discharged well 2 weeks later
- Culture and sensitivity: no growth
- Currently patient is under follow up for bilateral renal calculi
Recent Comments