
Case contribution: Dr Radhiana Hassan
Clinical:
- A 61 years old, underlying DM, HPT, CKD stage IV.
- Presented initially with fever, abdominal pain and vomiting for 3 days.
- Clinically lethargy and septic looking and per abdomen examination showed tender at right lumbar region.
- UFEME showed presence of leukocytes
- She had one hypotensive episode during admission and treated as sepsis.
- Also noted acute on chronic renal failure
Ultrasound findings:
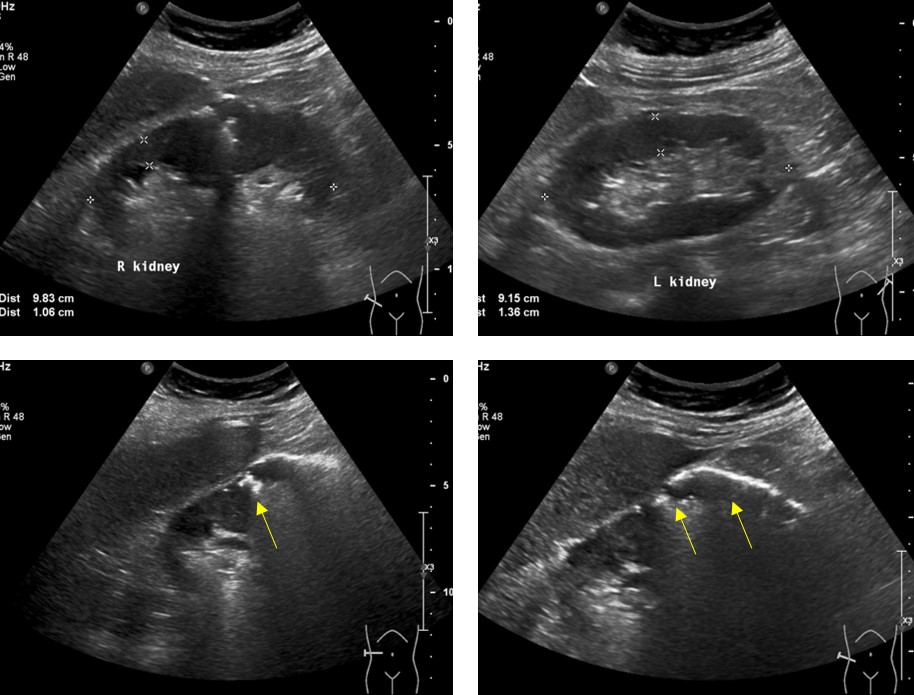
- The right kidney is slightly enlarged with poor corticomedullary differentiation.
- There are linear air shadows in the interpole and lower pole region of the right kidney (yellow arrows).
- Left kidney showed increased echogenicity. It measures 9.2 cm in bipolar length with cortical thickness of 1.4 cm.
- No renal calculus or hydronephrosis seen bilaterally. No dilated ureters.
- Urinary bladder is partially distended with Foleys balloon in situ. No free fluid seen.
CT scan findings:
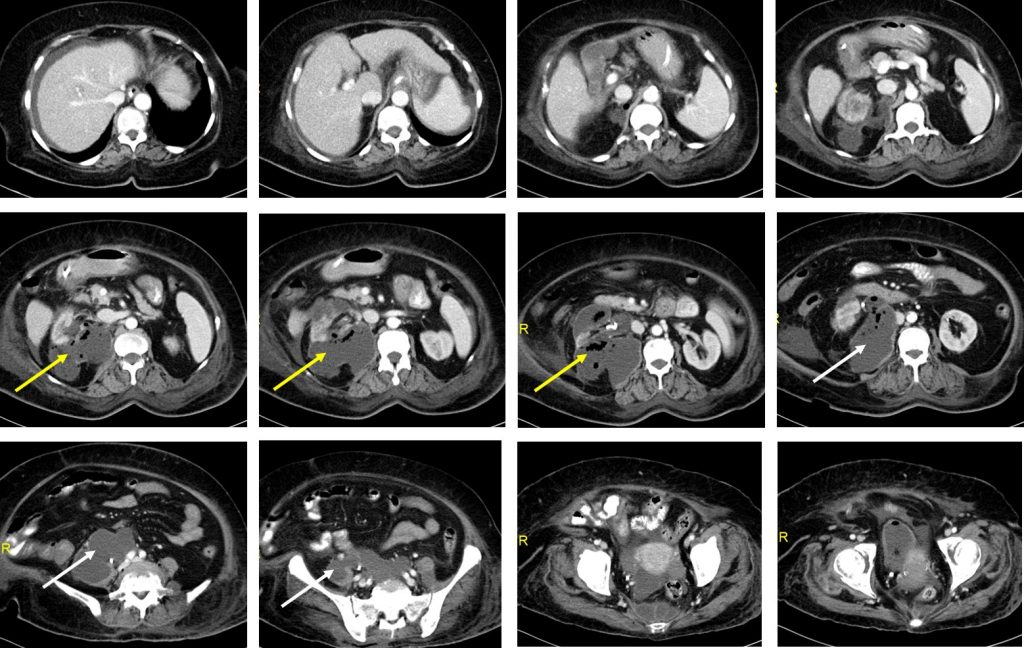
- The right kidney appears distorted and heterogeneous with normal enhancement of residual renal parenchyma.Streakiness of the right perinephric fat. There are thickening and enhancement of the right Gerota’s and Zuckerkandl fasciae.
- Presence of large peripherally enhancing perinephric collection extending from the right renal pelvis and lower pole region of the right kidney (yellow arrows). Multiple air pockets are seen within.
- The collection is extending posteriorly to the right psoas muscle and inferiorly until the presacral region (white arrows).
- It is collectively measured 9.8 x 8.2 x 15.6 cm (AP x W x CC) at the largest pool.
- Superiorly, it is abutting the medial limb of right adrenal gland. However no focal lesion is detected within. This collection is also abutting the inferior vena cava (IVC) anteriorly. No filling defect is seen within the IVC.
- Left kidney is normal in location and size.
- Urinary bladder is partially distended with Foleys catheter balloon in situ.
- No thickening or abnormal dilatation of the small bowel loop is identified. No enlarged intra-abdominal nodes.
Diagnosis: Emphysematous pyelonephritis
Discussion:
- A life threatening acute fulminant necrotizing infection of kidney and perirenal tissues associated with gas formation
- Acute and chronic necrotizing pyelonephritis with multiple cortical abscesses
- It can be bilateral in 5-7%
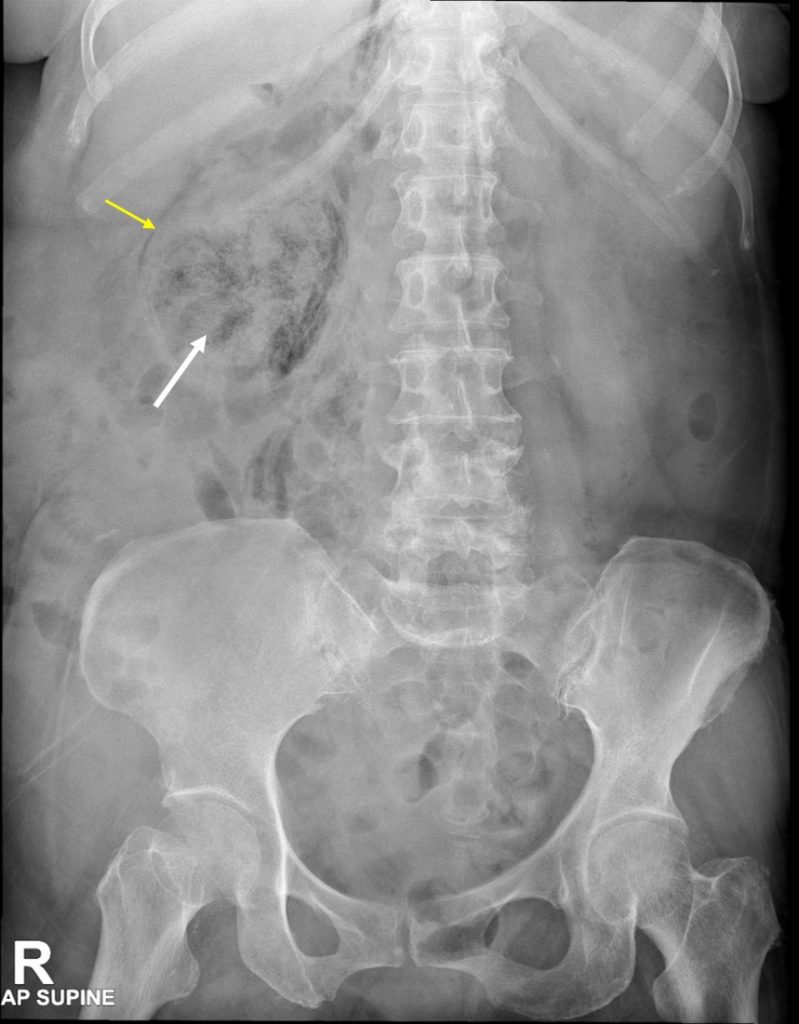
- Plain radiograph shows streaky or mottled appearance in renal fossa, crescent of subcapsular perinephric gas and linear gas along paraspinal region
- On CT scan, mottled areas of low attenuation extending radially along the pyramids can be seen. Extensive involvement of kidney and perinephric spaces and air extending through gerota’s fascia into retroperitoneal space
- Mortality rate 60-75% under antibiotic treatment
Progress of patient:
- CT guided drainage was performed
- A total of 60 cc pus drained
- Urine culture: Klebsiella pneumoniae
Recent Comments