
Case contribution: Dr Radhiana Hassan
Clinical:
- A 30 years old
- Presented with painful swelling of left breast
- No fever
- No family history of breast cancer
- Similar presentation few months ago which resolved spontaneously
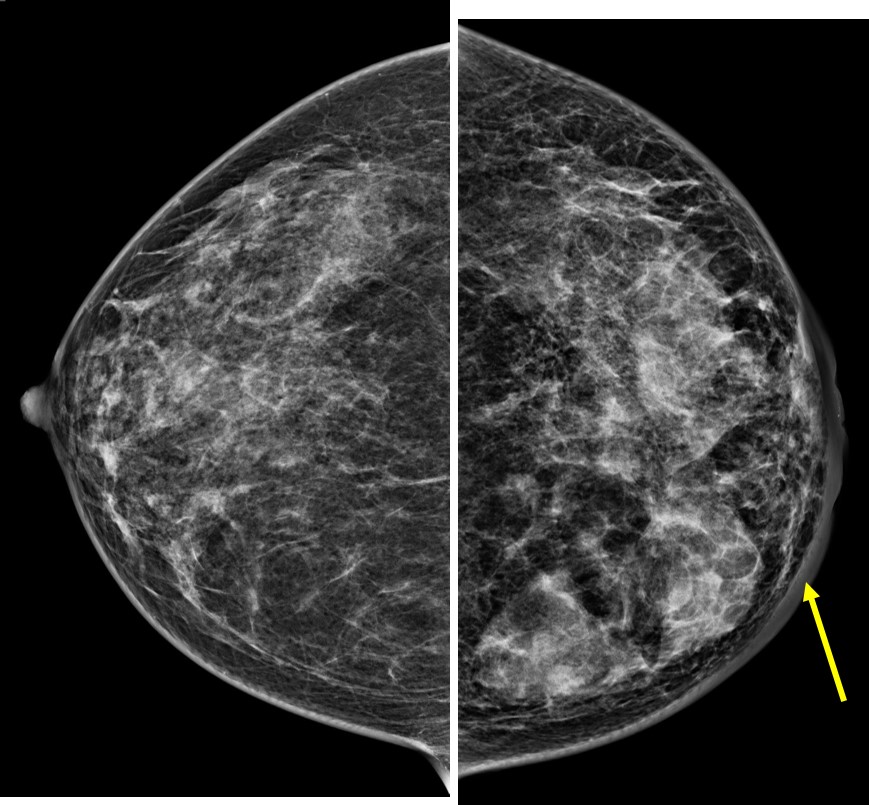
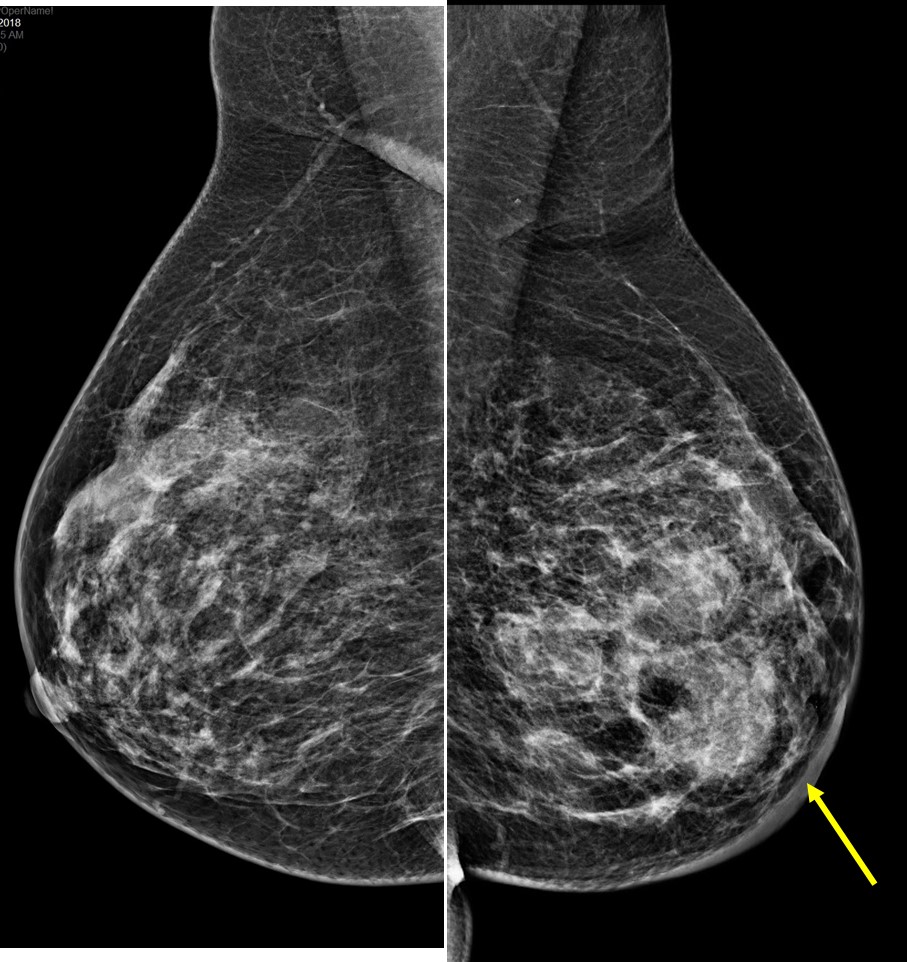
Mammogram findings:
- Bilateral dense breasts, BIRADS C
- Asymmetrical density and parenchymal pattern is seen
- There are multiple lobulated lesions on tomosynthesis images (not shown)
- Associated skin thickening is seen
- No stromal distortion, no nipple retraction
- No abnormal axillary node
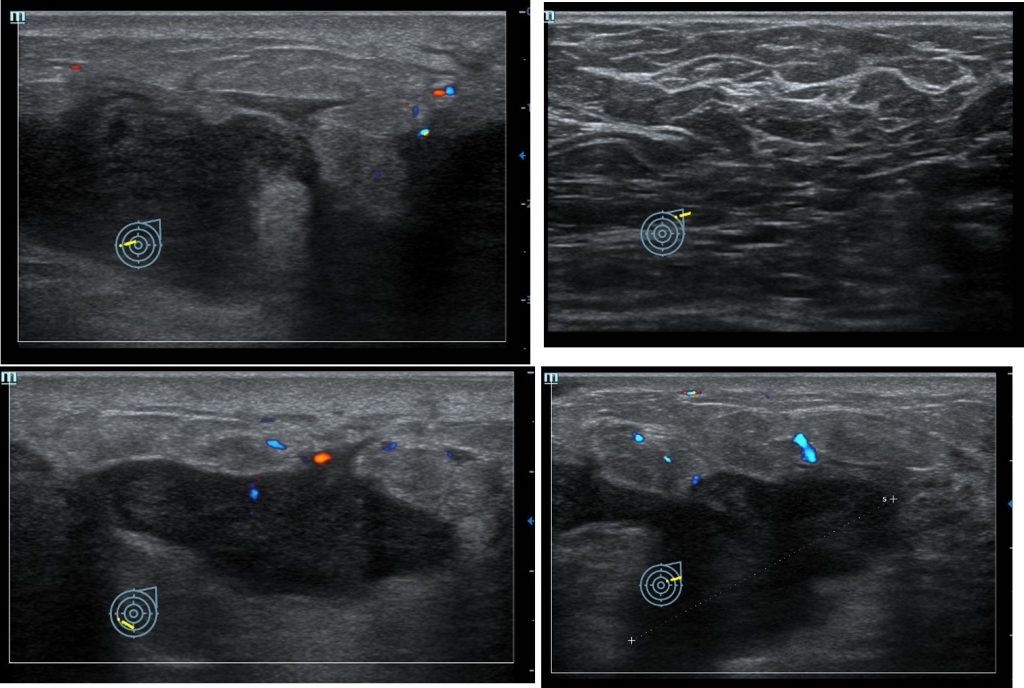
Ultrasound findings:
- There are multiloculated hypoechoic lesions with irregular outline
- In all quadrant of left breast with some infiltrative border
- No posterior shadowing
- Increased in surrounding vascularity
- Thickened and oedematous overlying subcutaneous fat and skin
- No abnormal axillary node is seen
Diagnosis: Granulomatous mastitis (HPE proven)
Discussion:
- Granulomatous mastitis is a rare chronic inflammatory disease of the breast.
- The most common presentation is unilateral breast mass often associated with inflammation of the overlying skin.
- Nipple retraction and a sinus formation may be present.
- Regional lymphadenopathy is present in up to 15% of cases.
- The most common finding is a focal asymmetry on mammography but is is not characteristic of this disease.
- On ultrasound it is seen as an irregular hypoechoic mass with tubular extension on ultrasound.
- On MRI, a focal or diffuse asymmetrical signal intensity without significant mass effect or nodular lesion can be seen. Enhancement pattern also varies and can differ from patient to patient and from lesion to lesion.
- Core biopsy is typically diagnostic.
- Differential diagnosis include inflammatory breast cancer, pyogenic mastitis/abscess, advanced breast cancer with lymphatic invasion and breast sarcoidosis (rare)
Recent Comments