
Case contribution: Dr Radhiana Hassan
Clinical:
- A 31 years old male
- Presented with headache and blurred vision
- Gradually worsened in 2 years
- No loss of consciousness, no vomiting, no seizures
- Clinical examination shows no significant neurological deficit except for reduced visual acuity of left eye
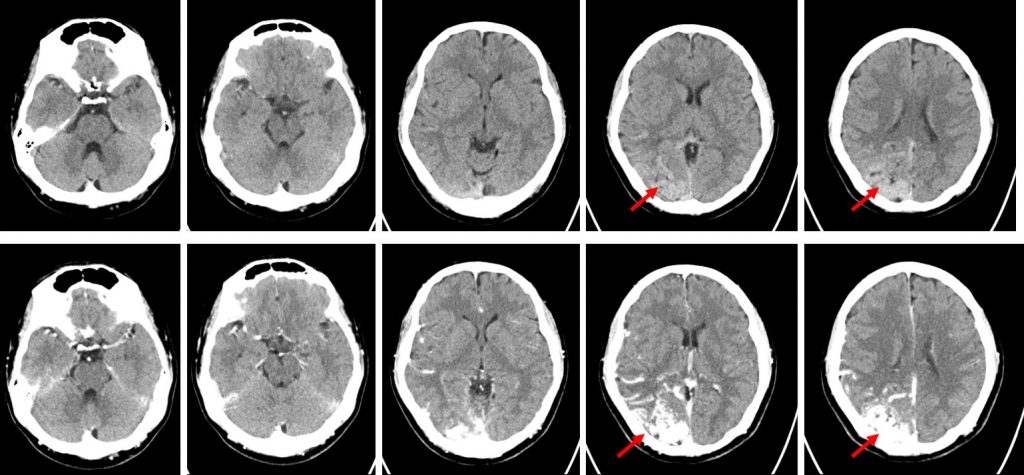
Plain and contrast-enhanced CT brain findings:
- A well-defined, hyperdense, intra axial, tubular serpenginous structures are visualised at the right parieto-occipital region which shows avid contrast enhancement similar to those enhanced intracranial vessels (red arrows) most likely represents a cerebral arteriovenous malformation.
- The nidus of the lesion measures at approximately 2.5 cm (AP) x 4.3 cm (W) x 5.5 cm (CC).
- No associated intralesional calcification.
- No surrounding sulci effacement or parenchymal oedema.
- No erosion of overlying skull.
- The right middle cerebral artery is more prominent compared to the left side, with multiple dilated arteries supplying the nidus observed.
- Prominent and dilated cortical veins are noted.
- Grey and white matter differentiation is preserved. No abnormal leptomeningeal enhancement.
- No acute intracranial bleeding. No midline shift or significant mass effect.
- Ventricles are not dilated. Cerebral sulci, extra-axial CSF spaces and basal cisterns are not effaced.
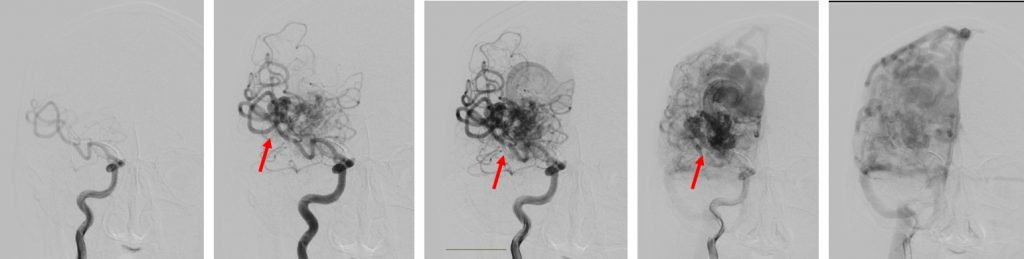
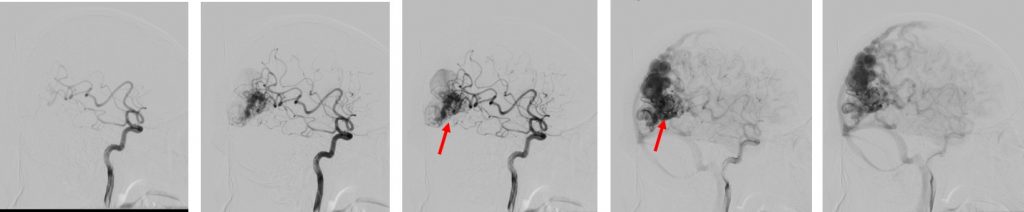
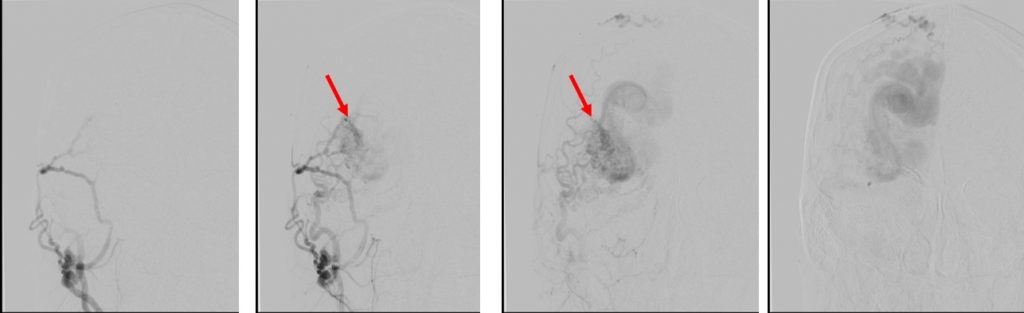
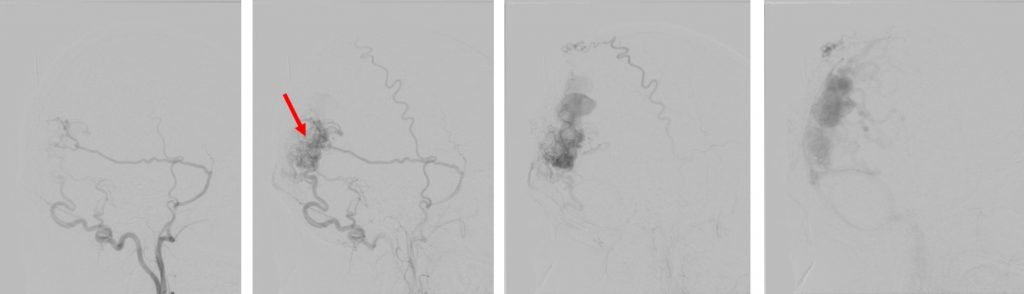
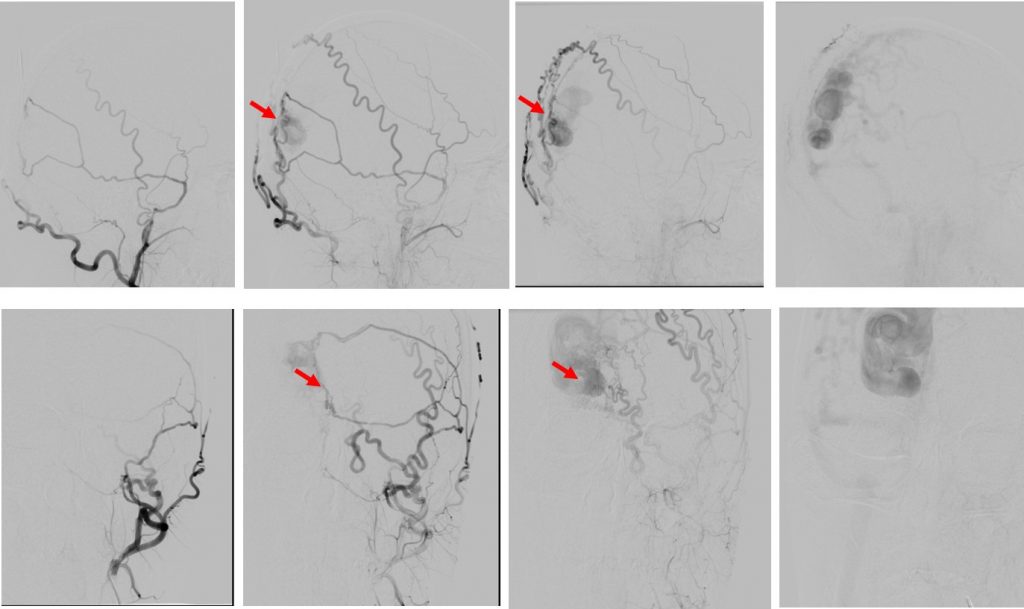
Cerebral angiogram findings:
- There is a large serpenginous dilatations of vessels seen in the right parieto-occipital region, representing the nidus of an arteriovenous malformation. The nidus measures 3.8 x 2.0 cm.
- It appears to receive arterial supply predominantly from the right middle cerebral artery (MCA), right posterior cerebral artery (PCA), and occipital and middle meningeal arteries of both external carotid arteries (right and left).
- It is seen draining into the superior sagittal sinus and transverse sinus with large dilated and tortuous cortical veins seen medially. No drainage to the deep venous system apparent.
- Multiple intranidal aneurysms are observed within.
- No other evidence of vascular malformation or aneurysm in the other parts of the brain.
- Large right parieto-occipital arteriovenous malformation with multiple internal and external carotid arteries feeders and multiple intranidal aneurysms. Spetzler-Martin grade 3 (size =2, eloquence = 1).
Diagnosis: Brain AVM.
Discussion:
- Brain AVM is a pial vascular malformation with direct artery and venous shunting with no intervening capillary bed
- It may occur anywhere in the brain but supratentorial location seen in 85% and posterior fossa in 15% of cases
- It is usually solitary and sporadic. Multiple AVMs are rare and usually syndromic
- Size varies but mainly 3-6 cm
- Morphology: enlarged feeding arteries, nidus of tightly packed enlarged vascular channels and dilated draining veins
- About 27-32% have dual arterial supplies from pial and dural
- No normal brain in between with minimal or no mass effect.
- CT scan shows calcification in 25-30% of cases
- Bleeding AVM (parenchymal and intraventricular are more common than subarachnoid hemorrhage)
- MRI is described as tightly packed serpentine flow void vessels with little or no brain tissue inside the nidus. May have some high signal in the brain due to gliosis
- Vivid enhancement on post contrast CT scan or MRI
- Classification based on Spetzler-Martin scale:
- Size- small <3 cm =1, medium 3-6 cm =2 and large >6 cm =3
- Location: noneloquent area =0, eloquent areas=1
- Sensorimotor cortex
- Visual cortex
- Hypothalamus and thalamus
- Internal capsule
- Brain stem
- Cerebellar peduncle
- Deep nuclei
- Venous drainage; superficial only =0, deep=1
Recent Comments