
Clinical:
- A 38 years old lady
- Progressive abdominal distension over 3 months
- Associated with loss of appetite
- No bowel related symptoms
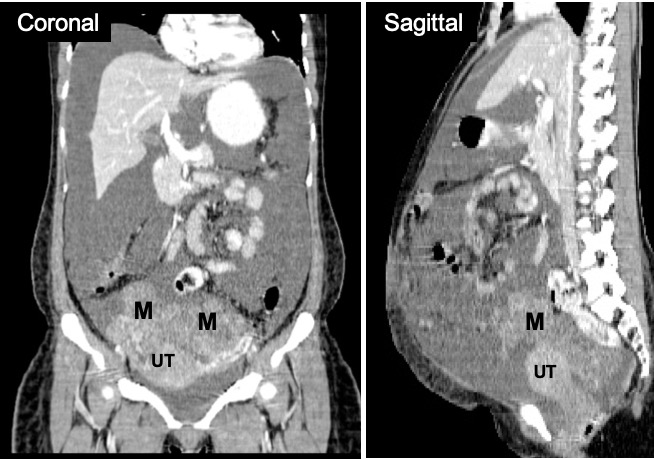
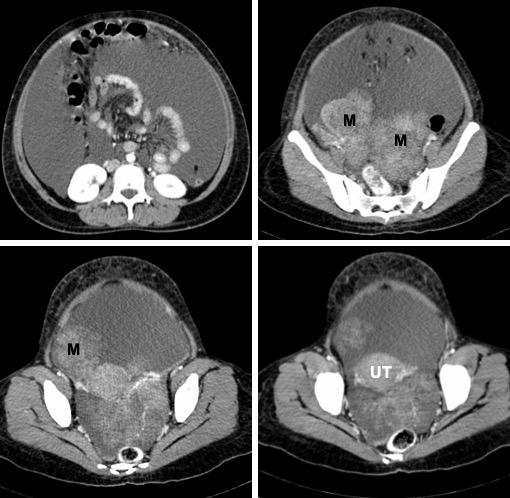
CT scan findings:
- Lobulated soft tissue mass at pelvic region (M), poor outline with uterus (UT)
- Both normal ovaries are not seen
- No calcification or fat component within the lesion
- Heterogenous enhancement post contrast
- Massive ascites
- All other organs are normal
Intra-operative findings:
- Gross ascites, straw coloured about 5.0 L
- Both ovaries showed fungating tumour 8x8x7 cm, fragile
- Both fallopian tubes normal
- Uterus normal
- Cervix and vagina normal
- Omentum free of deposits
HPE findings:
- Macroscopy: The left ovarian tumour measures 105x80x70 mm in diameter. The capsule is ruptured with multiple fungating solid mass and papillary structures seen. Cut section of the tumour shows solid tumour with area of hemorrhage. A few cystic spaces are also seen measuring 8-20 mm containing jelly like material. There are multiple fragments of detached tumour measuring 100 mm in aggregate diameter. Part of right ovary measures 40x15x10 mm.
- Microscopy: Sections from left and right ovarian tumours shows malignant cells arranged in closely packed papillary structures with delicated fibrovascular cores. The cells have pleomorphic vasicular nuclei with prominent nucleoli. Many mitotic figures and tumour necrosis are seen. Stromal invasion is evident and and the tumour is seen invading the capsule. Similar tumour implants are noted on the serosal surfaces of the uterus and right FT.
- Interpretation: Bilateral serous adenocarcinoma with malignant tumour implants seen on the serosal surface of the uterus and right fallopian tube.
Discussion:
- Imaging features of ovarian neoplasm virtually never allows a specific diagnosis
- Signs suggestive of malignancy include
- solid non-fatty non-fibrous tissu component
- many solid elements in a complex lesion
- wall thickness > 3 mm
- inner wall irregularities or papillary projections
- thick septations > 3 mm
- Increased echogenicity within a cyst
- ascites
- More than one third of ovarian cancer patients present with malignant ascites at diagnosis; additionally, development of ascites is a fundamental part of chemoresistant and recurrent disease
- The onset and progression of ascites is associated with poor prognosis and deterioration in the quality of life of patients
- The term “malignant ascites” is commonly used when the tumor fluid is tested positive for malignant cells and has a high level of lactate dehydrogenase, suggesting that the ascites may contain tumor cells with rapid proliferative rates indicative of rapid progression of the disease.
Recent Comments