
Clinical:
- A 26 years old lady
- Right distal thigh swelling for one year
- Recent increase in size
- Associated with dull pain on and off
- Worsening of pain upon prolong ambulation
- No constitutional symptoms
- Clinically examination shows a mass over medial aspect of distal femur about 8×6 cm, bony hard and non-mobile, not attached to skin. No skin changes.
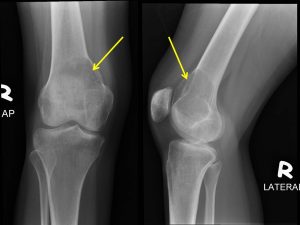
Radiographic findings:
- There is an expansile lytic lesion at metaphysis of distal femur
- It showed narrow zone of transition, No obvious sclerotic margin
- Thinning of the cortex
- “soap-bubble” appearance seen
- No fracture
- No obvious soft tissue swelling
- No extension to articular surface
- No periosteal reaction
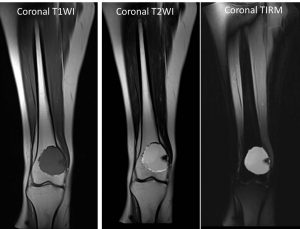
MRI findings:
- A well defined fairly round lesion noted at distal right femur. The lesion measure 3.8 x 4.7 x 4.6cm (APxWxCC). It is located about 1 cm from knee joint.
- The lesion appears hypointense on T1, hyperintense on T2 and not suppressed on FLAIR.
- It has well defined irregular margin which appear hypointense on T1 and T2WI.
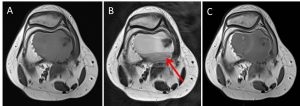
- Multiple thin septation within which enhanced post contrast. The peripheral of the lesion also enhanced post contrast.
- Fluid-fluid level noted (red arrow).
- Normal signal of bone marrow surrounding the lesion. No cortical break or periosteal reaction. Surrounding muscles are normal. The neurovascular bundle is intact.
HPE findings:
- Macroscopy: specimens labelled as bone and cyst aspirate.
- Microscopy: Section of bone specimen shows fragmented unremarkable bony trabeculae and marrow spaces, admixed with a fragment of fibro-collagenous tissue. The marrow spaces are consist of fatty tissue and normal hematopoietic cells. The fibro-collagenous tissue are composed of bland fibroblast proliferation, aggregates of cholesterol clefts and occasional multinucleated giant cells. In areas, hemosiderin laden macrophages are also noted. Negative for malignancy.
- Section of tissues from cyst aspirate shows predominantly blood admixed with tiny fragments of fibro-collagenous. The fibro-collagenous tissue are composed of bland fibroblasts proliferation and scattered multlinucleated giant cells. In areas, hemosiderin laden macrophages are also noted. Negative for malignancy.
- Interpretation: compatible with aneurysmal bone cyst
Diagnosis: Aneurysmal bone cyst
Discussion:
- Aneurysmal bone cysts are benign expansile tumor-like bone lesions of uncertain etiology mostly diagnosed in children and adolescents
- Peak age 16 years; range from 10-30 years, in 75% <20 years
- Female>Male
- Location
- Spine: 12-30%, predilection for posterior elements. Thoracic>lumbar>cervical spine
- Long bones: eccentric in metaphysis of femur, tibia, humerus, fibula
- Radiographic features include:
- Purely lytic eccentric radiolucency
- Aggressive expansile ‘soap-bubble’ pattern with internal trabeculations
- Sclerotic inner portion
- Almost invisible thin cortex
- Tumour respect epiphyseal plate
- No periosteal reaction
- CT shows blood-filled sponge with fluid-fluid levels
- MRI shows
- multiple cysts of different signal intensity representing different stages of blood products
- Low signal intensity rim = intact thickened periosteal membrane
- Angio: hypervacularity in lesion periphery in 75%
- Bone scan: ‘doughnut sign’= peripheral increased intake and a photophenic centre
Progress of patient:
- Planned for extended curretage, bone cement and locking plate distal right femur
Recent Comments