
Clinical:
- A 44 years old lady
- No known medical problem
- Presented with odynophagia and dysphagia for 4 days after history of foreign body ingestion (accidentally swallowed fish bone)
- Associated with mild fever
- Clinical examination showed left lateral neck swelling
- Scope showed prominent posterior pharyngeal region
CT findings:
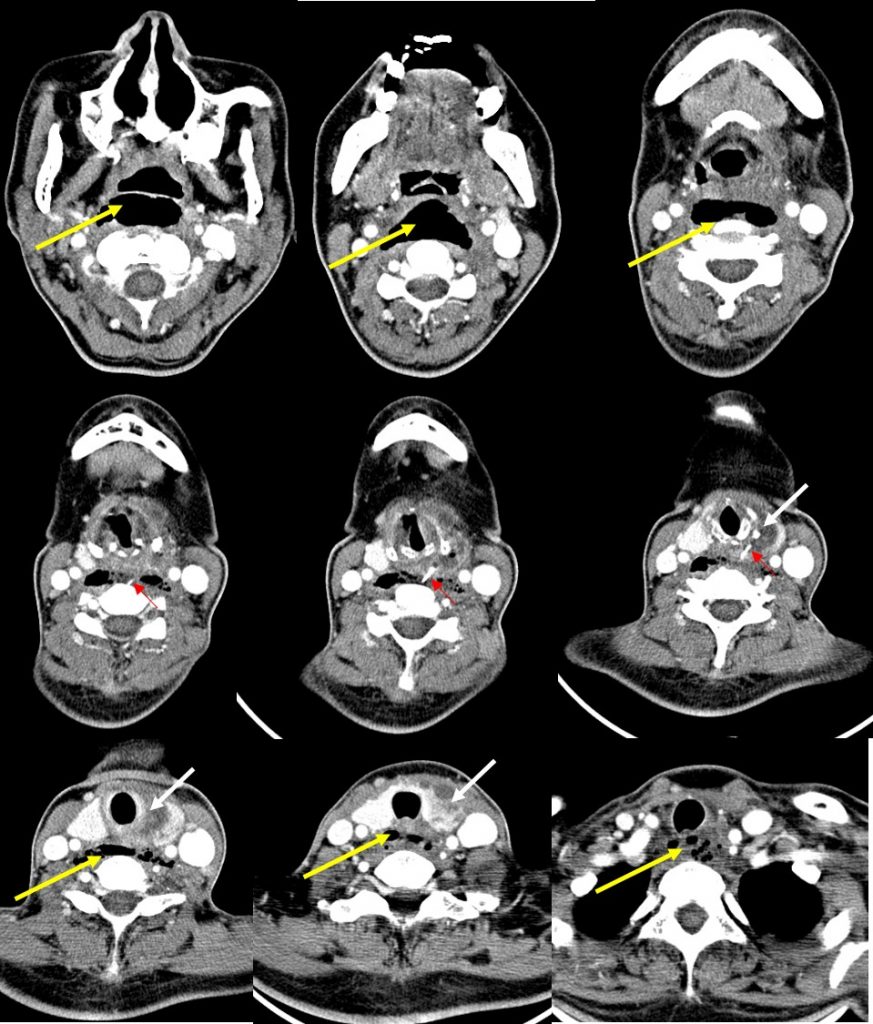
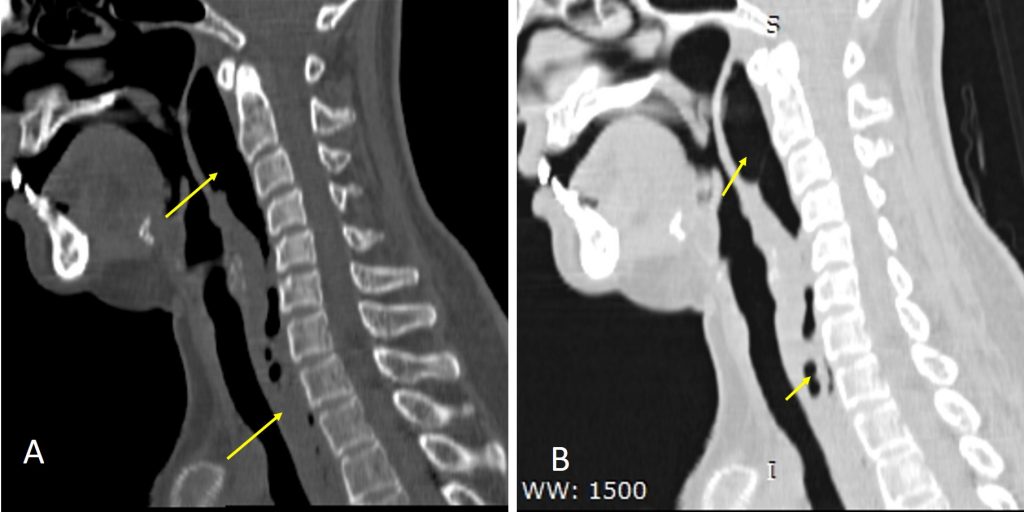
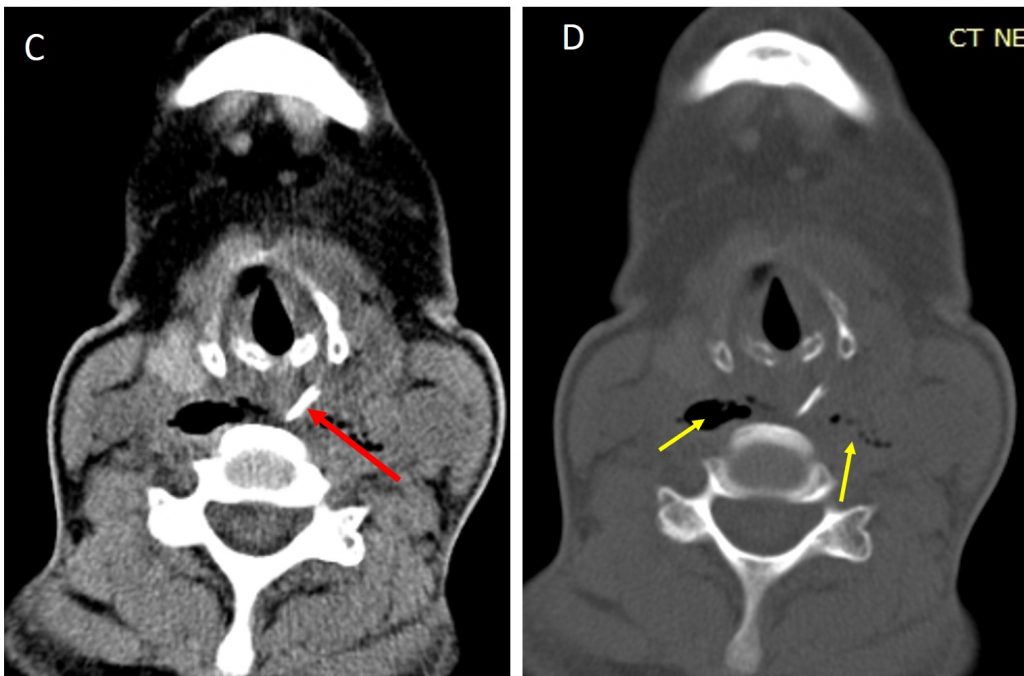
- There is a foreign (red arrow) body within the retropharyngeal space anterior to C5 vertebral body. This foreign body is dense with similar density to the bone. It is wedge-shape measuring about 14 mm in length and 7 mm at its base. The sharp end pointing posteromedially towards the vertebral body. Another end is seen piercing the through the left thryroid gland causing heterogeous swelling of the gland and the overlying strap muscles (white arrows).
- There is associated thickening of the retropharyngeal space from C1 to superior mediastinal region. The space measured 20mm at C2, 15mm at C6 and 13mm at T2 levels in thickness. There are air pockets seen within this spaces (yellow arrows).
- There is asymmetry of the piriform sinus with the left side seems to be obliterated. Small nodes are seen at submental, submandibular, upper and middle part of the jugular chain.
Diagnosis: Retropharyngeal abscess
Discussion:
- The retropharyngeal space is posterior to the pharynx and esophagus and anterior to the prevertebral muscles. It is bound by the visceral fascia anteriorly, the prevertebral fascia posteriorly, and the carotid sheaths laterally.
- The space extends from the clivus to the posterior mediastinum inferiorly atbthe level of diaphragm.
- Retropharyngeal abscess can occur due to ruptured suppurative retropharyngeal node, spread of infection from contiguous spaces across the fascial boundaries or direct inoculation from penetrating trauma (as in this case).
- The typical clinical presentation of retropharyngeal abscess is acute to subacute onset of neck pain, dysphagia or odynophagia, and a low-grade fever.
- CT findings of retropharyngeal abscess include
- pus fills the retropharyngeal space from side to side.
- retropharyngeal abscesses have an oval or rounded configuration;
- moderate-to-marked mass effect and it can produce anterior displacement of the pharynx and flattening of prevertebral muscles.
- The abscess usually has a thick enhancing wall
- Ancillary findings include evidence of primary infection or presence of a foreign body in traumatic causes.
- Possible complications such as airway obstruction, spread to danger space causing mediastinitis, pericarditis, pleuritis or vascular complications such as IJV thrombosis and pseudoaneurysm.
Recent Comments