
Clinical:
- A 36-year old man
- No known medical problem
- Presented with chronic headache and recent muscle weaknesses involving both hands.
- There was no history of trauma.
MRI findings:
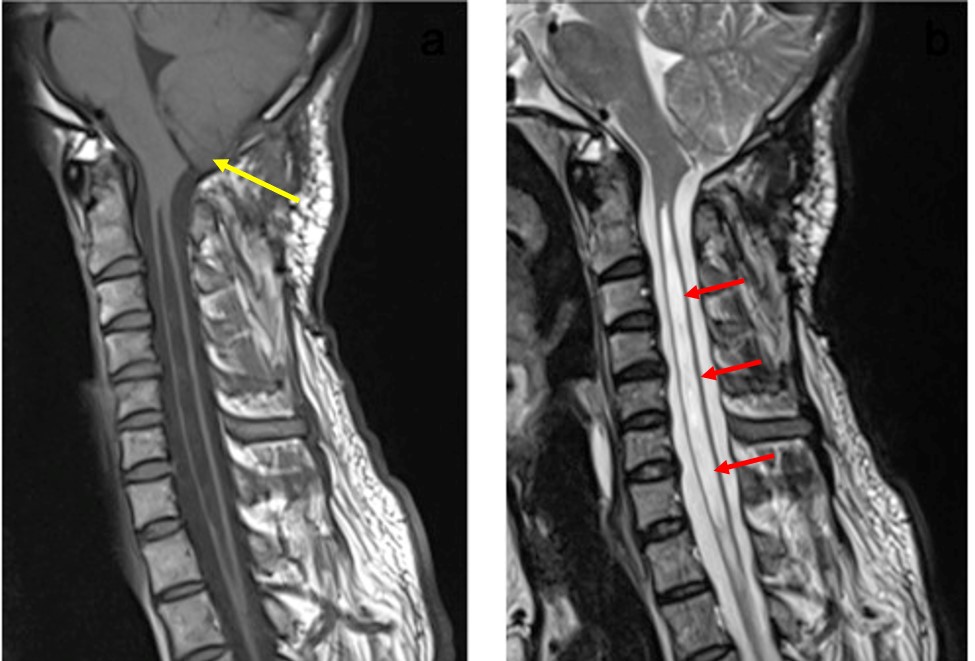
- MRI of upper spine in Sagittal T1 and T2 showed inferior herniation of the cerebellar tonsil about 6mm into the foramen magnum (yellow arrow).
- There was expansion of cervical and upper thoracic cord with associated lesion within the cord.
- The lesion seen is hypointense on T1 and hyperintense on T2-weighted sequences (red arrows).
Diagnosis: Arnold Chiari 1 malformation with syringohydromyelia.
Discussion:
- Chiari malformations are structural defects in the posterior fossa causing downward displacement of the cerebellar tonsils through the foramen magnum.
- It is divided into Type 1 to Type IV depending of the severity of the tonsilar herniation and associated abnormalities.
- The prevalence of Chiari 1 malformation was about one per 1000 births or higher.
- Women are more likely than men to have congenital Chiari malformation.
- Chiari 1 malformations are usually asymptomatic; however it may also cause various symptoms which include headache and those associated with syrinx or scoliosis.
- Syringomyelia can be associated with Chiari malformation type 1 and is commonly seen in the cervical cord. The exact mechanism of syringomyelia is unknown but many theories suggest that the herniated tonsils form an obstruction that does not allow an outlet of CSF from the brain to the spinal canal.
- Surgical intervention is based on occurrence of clinical symptoms rather than radiological findings.
- The presence of syrinx is an important indication that decompressive surgery is needed.
Recent Comments