
Clinical:
- A 6-year old boy presented
- Previously well and healthy
- Presented with fever, lethargy and poor oral intake for few days.
- Examination showed bilateral lower limb weakness and hypotonia.
MRI findings:
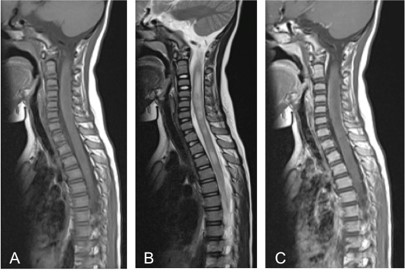
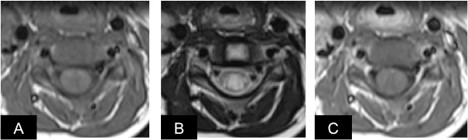
- MRI spine (A) T1WI, (B) T2WI and (C) T1 post contrast
- The MRI hows a long segment T2/STIR-hyperintense signal within the cords from C1 to C7, which was associated with cord expansion.
- Patchy involvement of the lower cord is also seen.
- The lesion involved more than two-third cross sectional area of the cord.
- The lesion does not enhanced on post contrast image.
- The vertebral bodies are normal.
Diagnosis: Acute transverse myelitis.
Discussion:
- Acute transverse myelitis is an inflammatory condition affecting both halves of the spinal cord and associated with rapid progressive motor, sensory and autonomic dysfunction.
- The incidence of acute transverse myelitis is 1-4 new cases per million people per year.
- It affects individuals of all ages with peaks at ages 10-19 years and 30-39 years.
- There is no sex or familial predisposition and usually there is no prior history of neurologic abnormalilty.
- Up to 40% of acute transverse myelitis may have normal MRI.
- In the remainder, MRI usually showed a long segment of T2 increased signal intensity. Commonly three to four segments were involved. On cross sectional image, the lesion is seen centrally located occupying more than two-thirds of the cross sectional area of the cord.
- The enhancement pattern is variable include no enhancement, diffuse, patchy or peripheral enhancement.
Recent Comments