
Clinical:
- A 54 years old man
- Background history of schizophrenia and hypertension
- Initial presentation with vomiting and unsteady gait
- CT scan shows cerebellar lesion
- Also noted to have lung lesion on chest radiograph
- Referred from other hospital for lung biopsy.
Radiographic findings:
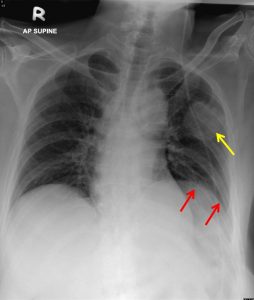
- There is a rounded well defined opacity seen at left mid zone (yellow arrow).
- No fluid level or cavitation within the lesion.
- No calcification of its wall or intralesional calcification noted
- No other lung lesion seen.
- No area of consolidation.
- No significant hilar or mediastinal enlargement.
- Elevated left hemidiaphragm (red arrows).
- Heart is not enlarged.
- No apparent suspicious lytic or sclerotic bony lesion seen.
CT scan findings:
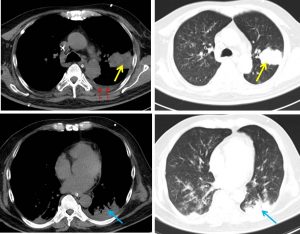
- A lobulated mass at apicoposterior segment of left upper lobe (yellow arrows)
- It shows well defined margin, no speculation
- It is peripherally located
- No intralesional cavitation, necrosis or calcification
- Patchy ground glass opacities in both lung fields
- Left pleural effusion (red arrows)
- Segmental collapsed consolidation of left lower lobe (blue arrows)
- A few mediastinal nodes are seen
HPE findings:
- Macroscopy: specimen labelled as lung biopsy consist of multiple pieces of greyish and whitish tissues
- Microscopy: Serial levels show malignant epithelial tumour arranges as nests and sheets with area of tumour necrosis. The tumour cells are moderate in size, ovoid to spindle in shape and have high nuclear to cytoplasmic ration. Nuclear moulding is identified. The chromatin is fine with salt and pepper appearance. The nucleoli are insconpicous. Mitoses are brisk including the mitotic figures. There is no glandular or squamous differentiation seen.
- Immunohistochemical staining: CK7, TTF-1, chromogranin, synaptophysin and P63 are all positive.
- Interpretation: Lung biopsy: small cell carcinoma
Diagnosis: small cell lung carcinoma
Discussion:
- Small cell lung carcinoma (SCLC) are neuroendocrine tumours of the lung
- Pulmonary neuroendocrine neoplasm includes typical carcinoid, which is a low-grade malignancy, atypical carcinoid, which is a medium-grade malignancy, and large cell neuroendocrine carcinoma and SCLC, which are high-grade malignancies.
- SCLC accounts for 15% to 20% of all lung cancers
- SCLC is more aggressive than non-small cell lung carcinoma (NSCLC) and is characterized by a rapid doubling time, high growth fraction (the ratio of proliferating cells to total cells), and greater propensity for early development of widespread metastases
- SCLC usually occurs in older men (60–70 years old) and is well known to be closely associated with smoking
- SCLC often present with a mass in or adjacent to the hilum and the tumour may well show mediastinal invasion (hilar tumors are defined as those where the center of mass was within or proximal to the lobar-segmental bronchial lumen)
- A noncontiguous parenchymal mass can be identified in up to 41% at CT that very rarely cavitates.
- Necrosis and hemorrhage are both common in SCLC.
- Most cases will present in advanced stages, be inoperable, and with a dismal prognosis.
- Cerebral metastasis are found in up to a quarter of patients at presentation 4 and are known as a common site of disease recurrence after an initial treatment response
- In this case, imaging findings are not characteristic of usual description for SCLC
Recent Comments