
Clinical:
- A 55 years old
- Presented with abnormal per vaginal bleed
- There is associated constitutional symptoms
- Ultrasound shows a complex cystic adnexal mass
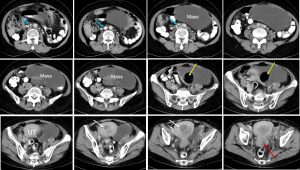
CT scan findings:
- There is multiseptated cystic mass on the left side with fat component. The cystic mass most likely from the left ovary, it extends inferiorly to be immediately lateral to the uterus/cervix. The mass measures 8x16x18 cm. The right ovary is not visualized.
- The normal urinary bladder is not visualized
- The uterus is enlarged with thickened enhancing wall measuring 8×9 cm. There is fluid in the uterine cavity. The lower uterus /cervix is bulky and shows abnormal enhancement. The segment shows ill-defined plane with the body of the uterus. The fat tissue around the uterus/cervix is streaky. The rectum has normal outline.
- Thrombosis of left femoral vein and common iliac vein
- There is IVC filter in-situ.
Intra-operative findings:
- Right ovary enlarged, 16x16x14 cm, multiloculated, ruptured during manipulation extruding clear fluid
- Left ovary seems to be normal
- Uterus enlarged to about the size of 18-20 weeks size of gravid uterus
- Parametria were infiltrated by the tumour bilaterally
- Bladder was also infiltrated by the tumour
- There were multiple tumour nodules in the POD size of about 1 cm, some on the lower part of the rectum
- There were multiple pelvic nodes bilaterally, largest being 2 cm in diameter on the right external iliac vein
- The paraortic nodes were not palpable.
HPE findings:
- Macroscopy: Specimen labelled as uterus, ovary, fallopian tube consists of uterus with left fallopian tube, left ovary and a remnant of right fallopian tube, a piece of ruptured ovarian cyst with attached fallopian tube. Cut section of the uterus show an irregular grey white tumour in the uterine wall measuring 40x30x20 mm. The anterior and posterior endomyometrium measure 30 mm and 40 mm respectively. The separated ovarian cyst measures 150x120x40 mm. It is a multiloculated cyst with no solid area seen. The locules are ranging from 15 mm ro 40 mm in diameter and filled with jelly like material and blood. No haemorhage necrosis seen.
- Microscopy: sections of the uterus show a malignant tumour infiltrating the myometrium and endometrium. At one area, the tumour has breached the serosa. The tumour is arranged as irregular and complex glands surrounded by chronically inflamed desmoplastic stroma. The glands are lined by stratified to single layer tall columnar cells having pleomorphic and hyperchromatic nuclei, prominent nucleoli and moderate amount of cytoplasm. In areas, the tumour cells are arranged as clusters and sheets. Mitosis is frequent. Tumour emboli are noted in the vascular channels. Atrophic endometrium is identified. Foci of malignant infiltration is seen in the bilateral fallopian tubes. The left ovary shows foci of malignant tumour with the morphology similar to the tumour in the uterus. The right ovarian cyst shows many cystic spaces lined by single layer tall columnar epithelium with basally located nucleus. In areas there are cystic spaces lined by cuboidal cells with intersprersed goblet cells and keratinized stratified squamous epithelial lining. A focus of malignant tumour is seen infiltrating the right ovarian tumour.
- Interpretation: Adenocarcinoma of the cervix, moderately to poorly differentiated with involvement of myometrium, uterine serosa, endometrium, bilateral ovaries and bilateral fallopian tubes.
- Left ovary: malignant infiltration seen, right ovarian cyst: mature cystic teratoma with malignant inifiltration
Discussion:
- Adenocarcinoma of cervix is a rare type of cervical cancer accounting for 10%–20% of all cervical cancers.
- The incidence of ovarian metastasis in early Stage Ib adenocarcinoma cervix is < 1%.
- The incidence of cervical adenocarcinoma with ovarian metastasis was associated more closely with tumor size.
- An author reported that approximately 5% of women with cervical adenocarcinoma are at an increased risk of ovarian metastases, which occurs in about half of ADC cases post-hysterectomy, thus oophorectomy is commonly performed to preclude OM.
- Ovarian preservation may be safely performed in young patients with early FIGO stage cervical adenocarcinoma without deep stromal invasion, endometrial invasion or perineural invasion, and particularly in the absence of uterine corpus invasion, parametrial involvement and infiltration to the vagina.
Recent Comments