
Clinical:
- A 55 years old man
- History of Benign prostatic hyperplasia
- Recurrent acute urinary retention with history of CBD insertion
- Hematuria and pain after last CBD insertion
Imaging findings:
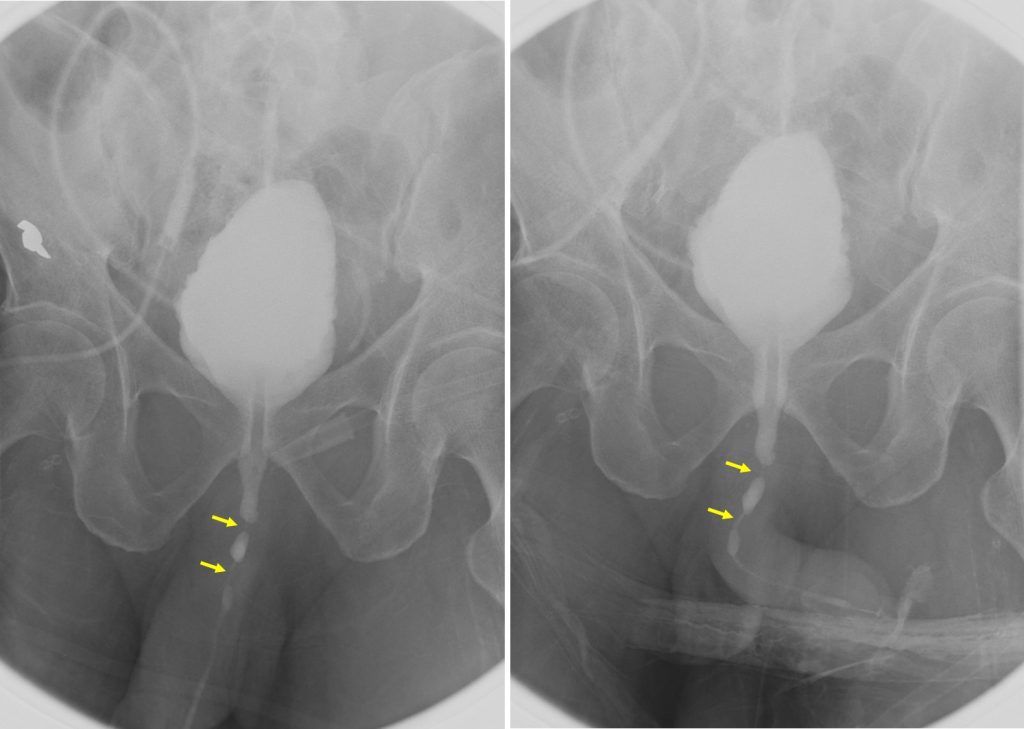
- Ascending and descending urethrogram performed
- Infusion of contrast into urinary bladder through the suprapubic catheter
- Urinary bladder is distended, margin is smooth and regular.
- Images taken during micturition.
- No outpouching or filling defect within
- No reflux of contrast into ureter or pelvicalyceal system
- Ascending urethrogram performed after that
- There is narrowing at anterior urethra with ballooning dilatation of urethra proximal to the stricture site. Two sites of narrowing identified (yellow arrows)
Radiological diagnosis: Anterior urethral strictures
Discussion:
- Urethral stricture is relatively common and usually involving male patients.
- Common causes include infection, inflammation, trauma, iatrogenic due to instrumentation or prolonged catheterization and congenital
- It is usual practice for patients with lower urinary tract symptoms to have their urinary flow rate measured as part of initial investigation. In those who have a urethral stricture the peak flow rate is typically low but the flow pattern is characteristically flat.
- Retrograde urethrography is the primary imaging used to assess urethral stricture. In certain cases, simultaneous antegrade cystourethrography and retrograde urethrography are often required to determine the length of the urethral defect.
- Ultrasound evaluation may show a thickening of the bladder wall associated with longstanding outflow obstruction, and a presence of residual urine. If these two signs are present, an ultrasound scan of the kidneys should be the next step to look for signs of obstructive uropathy.