
Case contribution: Dr. Raja Rizal Azman
Clinical:
- A 41-year old man with a history of diabetes and hypertension
- Presents with a one week history of worsening right sided upper and lower limb weakness and a single episode of facial twitching.
- Examination revealed a right sided upper and lower limb weakness with increased tone and brisk reflexes.
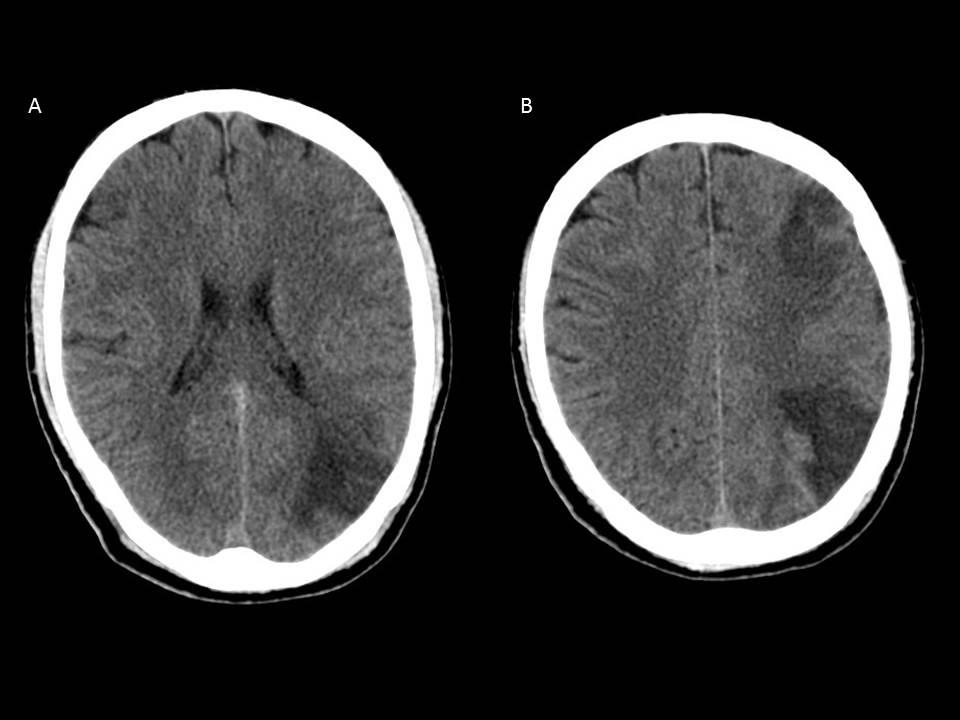
Imaging findings:
- Unenhanced CTof the brain at the level of the corona radiata (A) and the centrum semiovale (B)
- There are ill defined hypodensities affecting the grey and white matter at the left frontal lobe at the left MCA/ACA borderzone and the left parietal lobe at the MCA/PCA bordezone.
Diagnosis: Cortical watershed infarcts
Discussion:
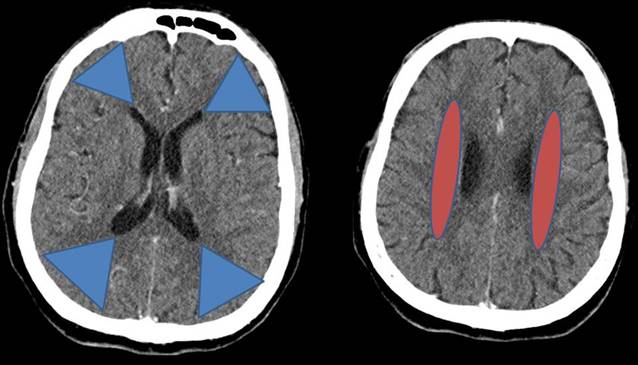
- Watershed infarcts occur at the borderzone of two vascular territories and represent up to 10% of infarcts.
- They can be classified into internal or cortical watershed infarcts.
- Internal watershed infarcts are thought to be secondary to haemodynamic compromise and have a risk of recurrent stroke with higher mortality and morbidity whereas cortical infarcts are more related to emboli and are associated with a more benign course.
Recent Comments