
Case contribution: Dr Radhiana Hassan
Clinical:
- Day 8 of life baby boy
- Born term, SVD
- Uneventful antenatal history
- Presented with persistent vomiting for one day duration
- Initially milk and fluid, latest greenish in colour
- Clinical examination shows no significant finding
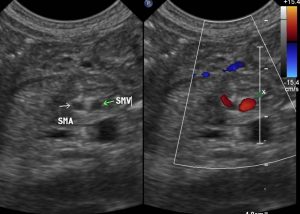
Ultrasound findings:
- There is SMA/SMV relationship inversion
- The SMA is on the right and the SMV is seen on the left side relative to each other.
- No whirlpool sign. No free fluid seen.
- No obvious thickening seen at pyloric region.
- Visualised solid organs are normal.
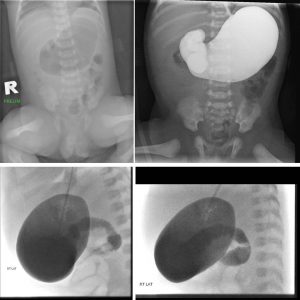
Flouroscopy findings:
- Preliminary film: Distended stomach with Ryle’s tube seen within. Distally located bowel gas is observed within the left side of the abdomen.
- About 50 cc of LOCM 1:1 dilution was introduced through the pre-inserted Ryle’s tube. Under intermittent fluoroscopy, flow of contrast is examined.
- Contrast is seen within the distended stomach.
- Smooth flow of contrast is only seen until the the 1st and 2nd part of the duodenum.
- However despite positioning and allowing some time, the contrast did not flow into the D3. Peristaltic motion of the opacified duodenum is observed, but with no significant propulsion of the oral contrast into the more distally located D3 observed.
- A ‘windsock’ appearance is observed, with intermittent bulbous duodenal dilatations which appear to subsequently subside.
- No opacification of D3 and D4 of the duodenum. Duodeno-jejunal (DJ) junction is not opacified even on delayed image.
- Reflux of contrast is also seen into the distal oesophagus.
Diagnosis: Malrotation (confirmed surgically)
Discussion:
- Intestinal malrotation is a congenital anatomical anomaly that results from an abnormal rotation of the gut as it returns to the abdominal cavity during embryogenesis.
- Intestinal malrotation is a congenital abnormality seen in up to 1:6000 live births
- Ultrasound may show an inversion in the SMA/SMV relationship with the SMA on the right and the SMV on the left. However, a normal SMA/SMV relationship can be seen in up to 29% of patients with surgically proven malrotation, whereas an inverted relationship is seen in up to 11% of patients.
- A more useful sign on ultrasound is demonstrating the retro-mesenteric D3 segment of the duodenum, where it is seen in a transverse plane between the superior mesenteric vessels and the aorta.
- Depending on the degree of malrotation, CT may show absence of a retro-mesenteric (retro-peritoneal) D3 segment of the duodenum, abnormal SMA (smaller and more circular)/SMV relationship, large bowel predominantly on the left and small bowel predominantly on the right and absence of D3 segment of the duodenum traversing the left of the spine.
- Upper GI study is the examination of choice when the diagnosis of malrotation is suspected. The key findings of malrotation is an abnormal duodenojejunal (DJ) junction location. On frontal view DJ junction lies inferior to the duodenal bulb and on lateral view the D2 and D3 segments of the duodenum is not located posteriorly in a retroperitoneal position.
Recent Comments