
Case contribution: Dr Radhiana Hassan
Clinical:
- A 45 years old man
- Underlying DM on oral medication
- Presented with productive cough for one week
- In ED, diagnosed DKA secondary to partially treated pneumonia
- Dxt= 16.6, HR=141 bpm, BP= 162/100mmHg, Temperature= 39.9°C

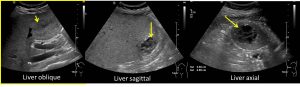
Ultrasound findings:
- There is hepatosplenomegaly.
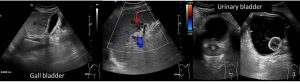
- Hypoechoic lesions are seen within the liver (yellow arrows) and spleen (red arrow) may represent abscess formation.
- Thickened gallbladder wall with pericholecystic fluid could represent cholecystitis.
- Slightly thickened urinary bladder wall with floating debris within urinary bladder may represent cystitis.
- No free fluid is seen.
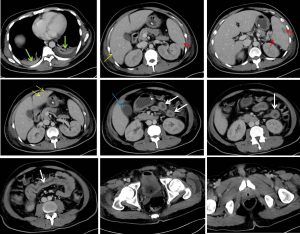
CT scan findings:
- Liver is enlarged measuring about 25.2 cm in craniocaudal length.
- Multiple small peripherally enhancing ill-defined multiloculated lesions with central low attenuation are identified in the liver suggestive of abscesses (yellow arrows).
- Ill-defined multiloculated non-enhancing hypodense lesion is also seen in the spleen suggestive of another foci of abscess formations (red arrows).
- The gallbladder is distended with thickened enhancing wall and pericholecystic fluid collection (blue arrow). No layering density within. No gallbladder calculus.
- Part of the small bowel wall appears slightly thickened with associated minimal surrounding fat stranding (white arrows). These possibly represent extension of inflammation.No bowel wall dilatation or perforation is seen.
- Pancreas is normal. Bilateral adrenals are normal. Prostate gland is also normal.
- Consolidation of bibasal lung with pleural effusion, more on the left side (green arrows)
Diagnosis: Meliodosis with multiorgan involvement.
Discussion:
- Meliodosis is an infectious disease caused by Burkholderia pseudomallei.
- The presenting symptoms are non-specific ranges from mild to severe illness.
- Humans are infected with B.pseudomallei by contact with polluted water.
- The infection is constantly present in Southeast Asia and northern Australia.
- Those with melioidosis are treated with a long course of antibiotics.
- Even if the disease is properly treated, approximately 10% of people with melioidosis die from the disease. If the disease is improperly treated, the death rate could reach 40%
- Diabetes is a major risk factor for melioidosis; over half of melioidosis cases are in people with diabetes.
- Imaging features depends on organ involvement:
- Pulmonary: multiple small pulmonary nodules (hematogenous spread) and multilobar infiltrates typically starting in the upper lobes. It can rapidly progress to cavitation or abscess formation.
- Head and neck: suppurative parotitis is seen and present as an abscess.
- Abdominal: Liver and spleen abscesses. Less commonly seen in pancreas, kidneys and prostate gland.
- CNS: cerebral abscess, cerebritis, encephalitis and dural venous sinus thrombosis.
Progress of patient:
- Initially admitted to ICU due to sepsis
- Obstructive jaundice due to acalculous cholecystitis
- Diagnosed meliodosis based on positive serology result.
- Treated with antibiotic, showed good response and discharged well
- Repeat CT scan one month later shows small residual abscesses in the liver and spleen.
Recent Comments