
Case contribution: Dr Radhiana Hassan
Clinical:
- A 60 years old lady
- Presented with left facial numbness
- Worsening over a few months
- Associated with occasional headache
- No hearing loss
- No constitutional symptoms
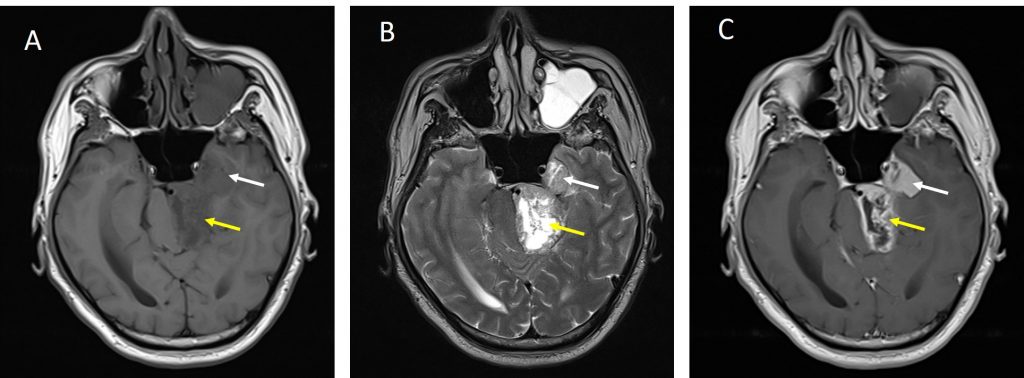
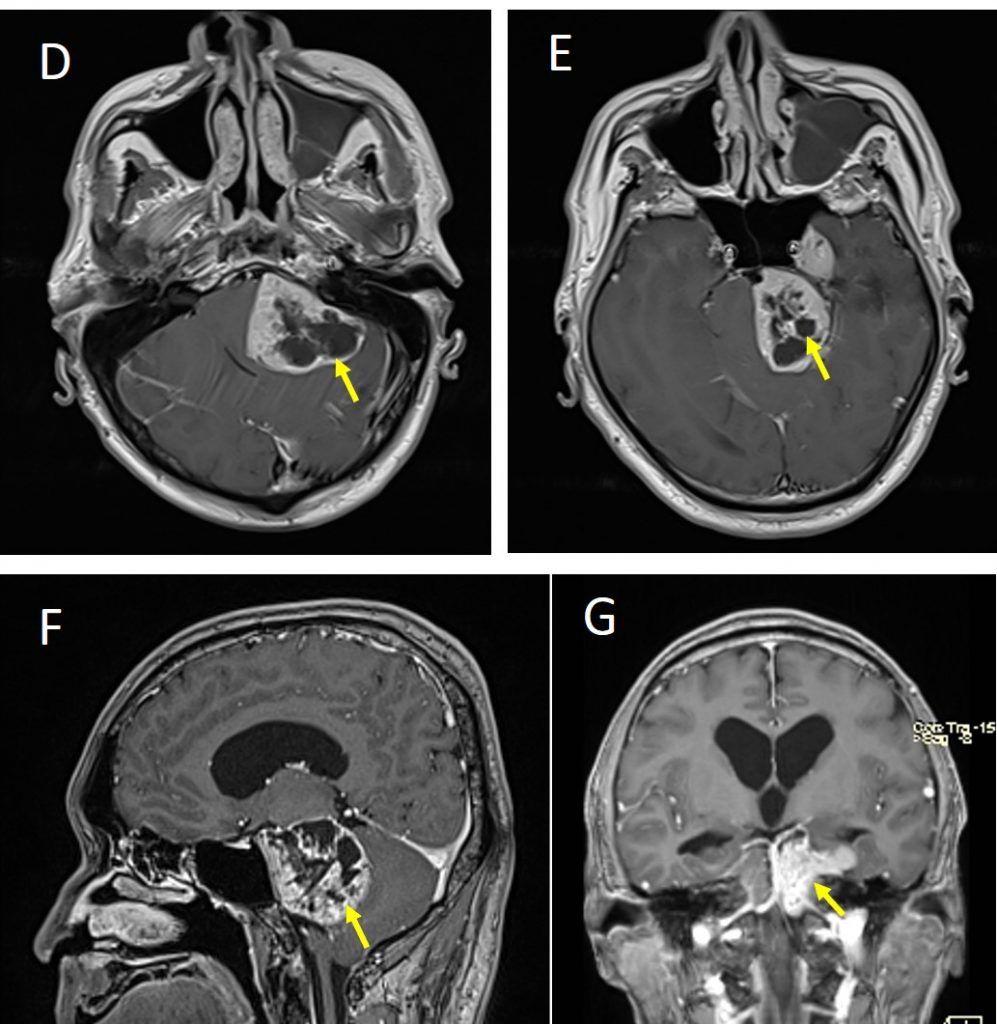
MRI findings:
- There is a lobulated mass at left cerebellopontine angle region (yellow arrows)
- The lesion is seen extending into left meckel cave (red arrows)
- No extension into the internal auditory meatus
- The lesion is heterogenously hypointense on T1, hyperintense on T2 and enhances heterogenously post contrast
- Significant mass effect is seen with compression of pons
- No hydrocephalus
Diagnosis: Trigeminal schwannoma (HPE-proven).
Discussion:
- Trigeminal schwannomas are the second most common intracranial schwannomas
- However the incidence remain uncommon being far less common than vestibular schwannomas.
- Patients usually presents at 3rd to 4th decades.
- They primarily arise from Schwann cells in the gasserian ganglion.
- Three major types of trigeminal schwannomas have been described based on the location; within the gasserian ganglion presenting as Mecke cave mass (most common), preganglion presenting as posterior fossa mass (second most common) and post ganglion presenting as infratemporal mass (less common).
- These lesions can also be unicompartmental or multicompartmental. A few classifications were proposed regarding radiologic findings on tumour location that have implications in planning the surgical approach.
- The radiological findings of a trigeminal schwannoma depends on the location of the tumor.
- Skull radiograph (if lesion is large) and CT scan may demonstrate bone changes which include erosion of the dorsum sellae or petrous apex and enlargement of outlet foramina such as the foramen ovale, foramen rotundum, or superior orbital fissure.
- On un-enhanced CT imaging, these lesions are usually isodense but can also reveal variable attenuation. Cystic areas (usually found in larger tumors) are hypodense, similar to CSF. Following administration of contrast they moderately enhance, often heterogeneously due to cystic areas.
- On T1W MRI, the lesion is typically isointense to brain, cystic areas appear hypointense. On T2W MRI, lesion is hyperintense to brain. Lesion in Meckel cave usually shows well demarcation. Post contrast image normally shows prominent heterogenous enhancement.
References/Suggested further reading:
- Trigeminal schwannoma at https://radiopaedia.org/articles/trigeminal-schwannoma
- Multicompartmental trigeminal schwannomas: Dumbbell tumours revisited. JCO Global oncology at https://ascopubs.org/doi/full/10.1200/JGO.2016.006122
Recent Comments