
Case contribution: Dr Radhiana Hassan
Clinical:
- A 30 years old lady
- No known medical illness
- Presented with vague abdominal discomfort
- Ultrasound shows cystic adnexal mass
CT scan findings:
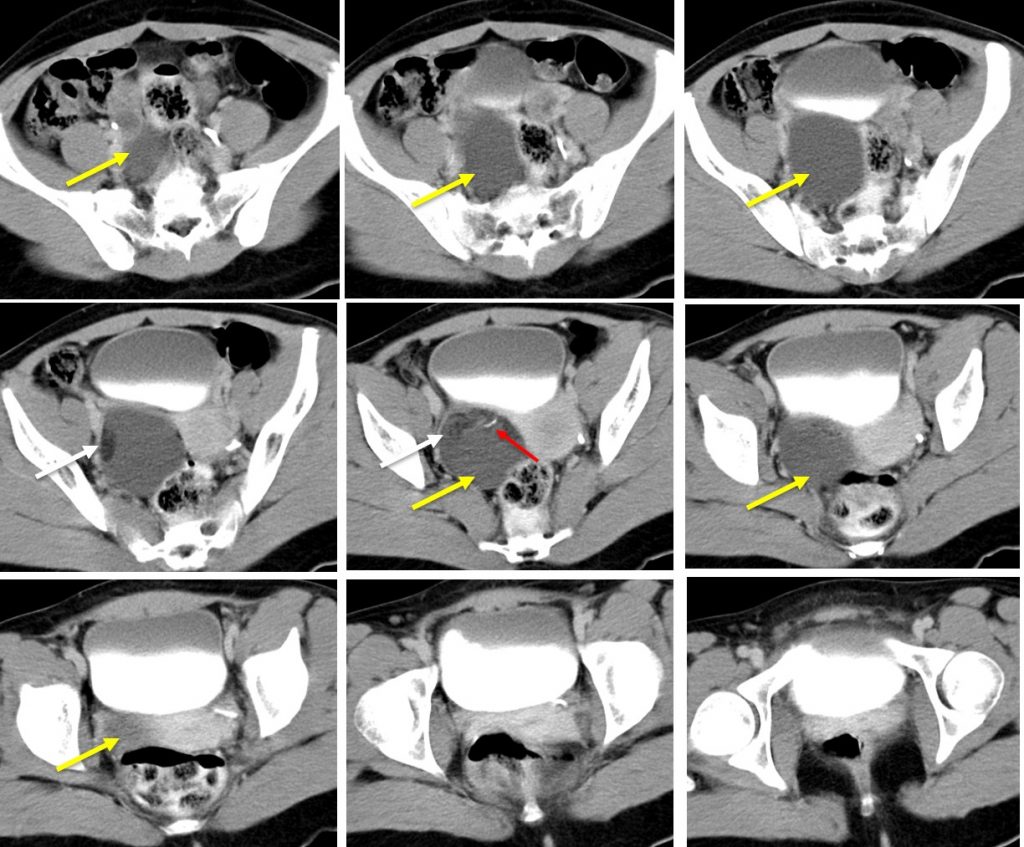
- There is a well-defined multiseptated mass posterior to the urinary bladder (yellow arrows). The mass is on the right side of uterus and has heterogenous density.
- It is mainly cystic with intralesional calcification (red arrows) and fat component (white arrows).
- The right pelvic ureter course lateral to the mass. The left pelvic ureter is normal.
- Uterus is grossly normal. No ascites.
Intra-operative findings:
- Right side ovarian cyst with intact capsule measuring 6×8 cm, ruptured during manipulation consist of mostly straw coloured fluid with small part of sebum gland and hair.
- Left tube and ovary are normal.
- No adhesion at POD. No ascites.
- Liver and peritoneum normal.
HPE findings:
- Macroscopy: specimen labelled as right ovarian cyst wall consists of a ruptured cysts measuring 80x25x10 mm, containing whitish material admixed with hair. The cyst wall is 1-3 mm in thickness. There is a solid area seen measuring 20x10x5 mm.
- Microscopy: section show ovarian cyst wall partly lined by keratine and non-keratinized stratified squamous epithelium and partly devoid of epithelium. The underlying stroma present of skin adnexa, adipocyte tissue, smooth muscle fiber, nerve bundle and seromucinous gland. No immature component or evidence of malignancy seen.
- Interpretation: Right ovarian mature cystic teratoma.
Diagnosis: Mature cystic ovarian teratoma
Discussion:
- Ovarian teratomas are the most common germ cell neoplasm.
- The most common of these tumors, the mature cystic teratoma (also known as dermoid cyst), typically contains mature tissues of ectodermal (skin, brain), mesodermal (muscle, fat), and endodermal (mucinous or ciliated epithelium) origin.
- Immature teratomas differ from mature ovarian teratomas both histologically by the presence of immature tissue, and clinically by their more malignant behaviour.
- Incidence:
- mature teratoma: account for about 10-20% of all ovarian neoplasms.
- Immature teratoma: less common, <1% of all ovarian teratomas
- Age:
- Mature teratoma: typically in young women, around the age of 30 year
- Immature teratoma: younger age group, mostly first 2 decades of life
- Pathology:
- Mature teratoma: They are composed of well-differentiated derivations from at least two of the three germ cell layers.
- Immature teratoma: presence of immature or embryonic tissue, as well as the mature tissue elements seen in a mature teratoma. The proportion of immature neuroepithelium present correlates with the tumour grade.
- Tumour markers:
- Mature teratoma: no raised in serum AFP, Ca125 +ve in 20-30%
- Immature teratoma: usually, does not produce beta-HCG, serum AFP elevated in 50-70%, Ca125 +ve in 50%
|
CT scan findings |
Mature teratoma | Immature teratoma |
| Bilaterally | Yes (10-15% of cases) | Yes |
| Size | Mean 6 cm | Mean 9 cm |
| Margin | Smooth,
well defined |
Irregular
Ill defined |
| Internal architexture | Mainly cystic | Solid or mixed |
| Mural nodule | Common | Not common |
| Fat component | Very common (93% of cases) | Common |
| Calcification | Distinct, sharp margin mainly in mural nodule, tooth-shaped (56% of cases) | Indistinct, small and scattered |
| Septum | Regular | Irregular |
| Local invasion | Nil | Yes |
| Distant metastasis | Nil | Yes |
Recent Comments