
Case contribution: Dr Radhiana Hassan
Clinical:
- A 77 years old male
- Presented with chronic cough for almost one year
- Associated with loss of appetite
- No fever. No hemoptysis
- Clinical examination shows mild clubbing and coarse crepitation at lower zones
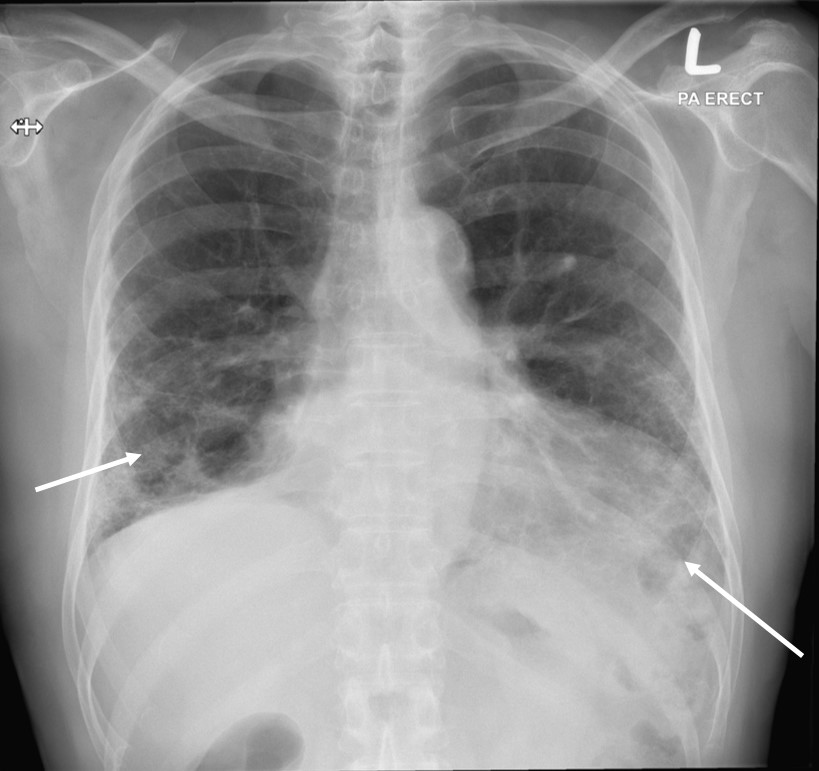
Radiographic findings:
- Reticular opacities seen predominantly at both lower zones (white arrows)
- Partial obliteration of right cardiac margin and left hemidiaphragm
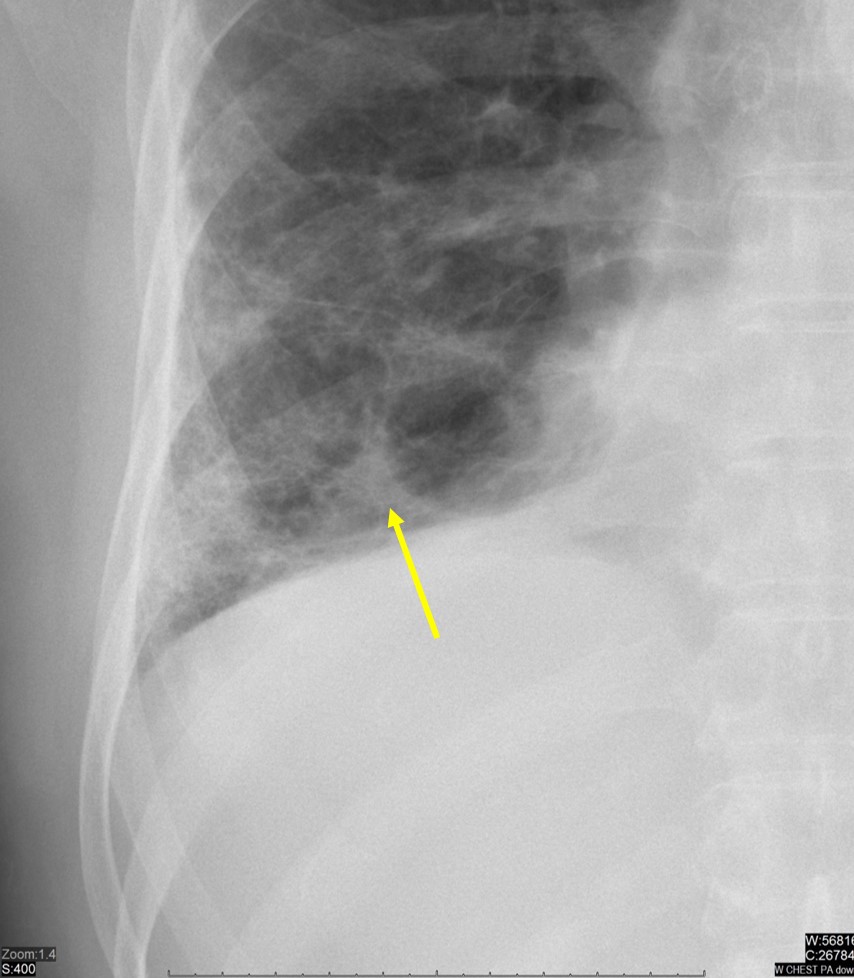
- An ill-defined nodular density is seen within the right lower zone (yellow arrow)
- Presence of cardiomegaly
- No pleural effusion. No hilar mass.
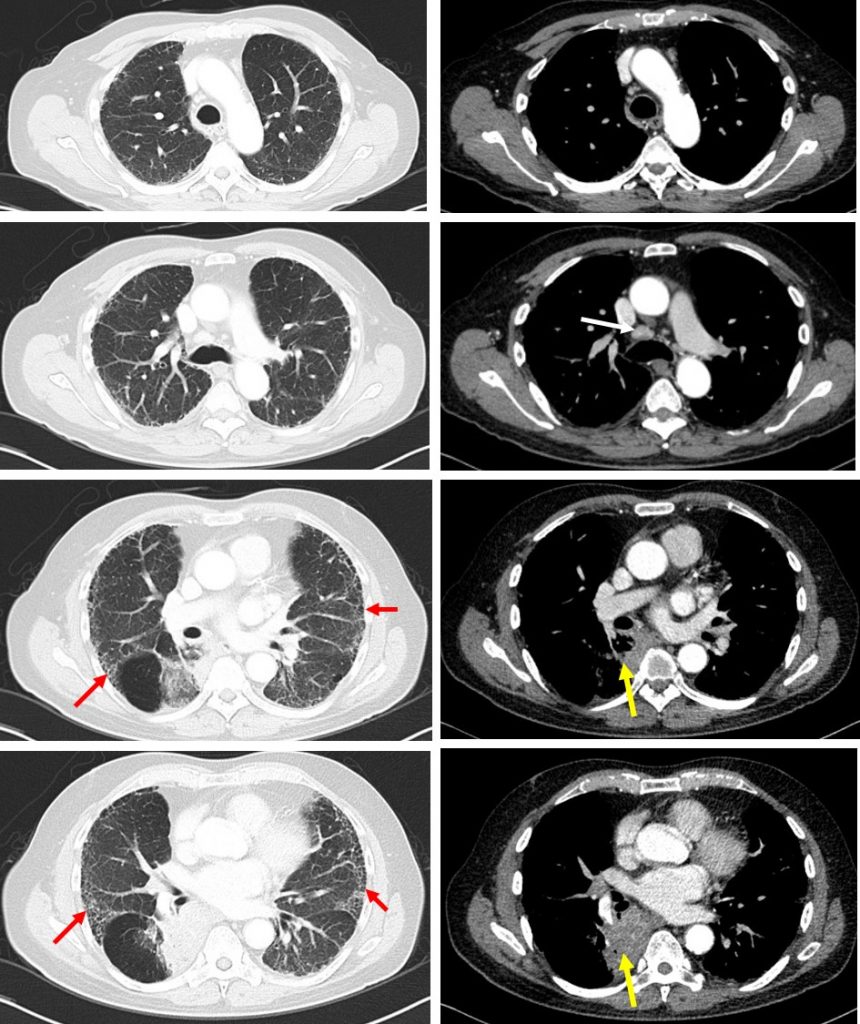
CT scan findings:
- There is segmental collapsed with mass involving the posteromedial segment of right lower lobe (yellow arrow) measuring about 5.8 x 3.7cm.
- No intralesional calcification. No cavitation.
- Honeycombing appearance in bilateral hemithorax (red arrows), mainly involving both lower lobes (left > right)
- Multiple lymph nodes are seen at the right paratracheal, precarina, subcarina and aortopulmonary windows. The largest is seen at the precarina region (white arrow), measuring about 11 mm.
HPE findings:
- Macroscopy: specimen labelled as right lower lobe lung mass.
- Microscopy: section shows 2 strips of tumour tissues composed of malignant cells infiltration, predominantly arranged in glandular architecture with some in sheets and clusters. The malignant cells display moderate pleomorphic, hyperchromatic to vesicular nuclei with prominent nucleoli and moderate amount of cytoplasm. Scattered mitosis are present. No necrosis noted. The surrounding tissue is mildly infiltrated by mixed inflammatory cells consisting of neutrophils, lymphocytes and plasma cells.
- Interpretation: adenomacarcinoma
Diagnosis: Lung adenocarcinoma in idiopathic pulmonary fibrosis.
Discussion:
- Idiopathic pulmonary fibrosis has been reported to be associated with increased risk of lung cancer as a result of the occurrence of atypical and dysplastic epithelial changes in fibrosis which progress to invasive malignancy.
- The incidence and clinical factors related to development of lung cancer are unclear.
- One study shows the cumulative incidences of lung cancer were 1.1% at 1 year, 8.7% at 3, 15.9% at 5, and 31.1% at 10 years.
- Risk factors of lung cancer were male gender, current smoking at IPF diagnosis, and rapid annual decline of 10% or more in forced vital capacity (FVC).
- Squamous cell carcinoma followed by adenocarcinoma was the most common histologic type.
- Lung cancer was frequently located in areas abutting or within fibrosis.
- Survival was significantly worse in patients with lung cancer compared to patients with IPF alone.
Recent Comments