
Case contribution: Dr Radhiana Hassan
Clinical:
- A 24 years old man
- Ulcerative colitis with poorly differentiated adenocarcinoma (T4N1M0)
- Subtotal colectomy with end ileostomy done
- Had perforated bowel during second chemotherapy
- Chest radiograph obtained after left central venous catheter insertion
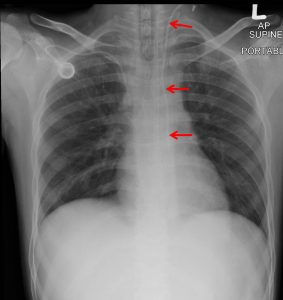
Radiographic findings:
- The left central catheter (red arrows) is seen traversing neck region to upper mediastinum and coursing inferiorly along the left side of paravertebral region
- The tip is at the level of T7
- No pneumothorax seen
- No widening of mediastinum
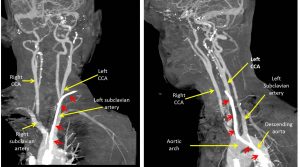
CT angiography findings:
- A catheter (red arrows) is seen traversing at the left neck straight into the left common carotid artery (at the level of thyroid gland).
- The distal tip seen within the descending aorta, about 4.3 cm below the carina level (from chest radiograph).
- No obvious haematoma is observed and no contrast extravasation on arterial phase is noted.
- The left internal jugular vein (IJV) is not opacified, in comparison to the right internal jugular vein. This is possible of left IJV thrombosis.
- A chemoport is observed with the port at the right upper chest subcutaneous tissue and the tip of the catheter in the superior vena cava just after branching into azygous vein. Endotracheal tube is seen with the tip around 5.5 cm above the carina.
- The visualized brain parenchyma is normal.
- The visualized lung apices are unremarkable. No pneumothorax.
Progress of patient:
- The patient was referred to vascular and team and the catheter was removed
- Point compression done for 5 minutes
- No complication post removal of catheter
Diagnosis: Inadvertent common carotid artery cannulation
Discussion:
- Multiple complications associated with central venous catheter insertion has been documented. The complications include arterial puncture, pneumothorax, neck or mediastinal haematoma and hemothorax.
- Obesity, short neck and urgent catheterisation are risk factors for complicated central venous insertion.
- Inadvertent carotid arterial puncture complication is reported in 2-8% of cases.
- Inadvertent carotid sheath insertion during central venous catheter placement could lead to serious complications such as airway obstruction, pseudo-aneurysm, arterio-venous fistula formation and retrograde aortic dissection.
- In the presence of occlusive (atheromatous) carotid disease, inadvertent puncture may carry the risk of precipitating a cerebrovascular accident.
- Treatment strategies after inadvertent arterial catheterisation include local compression, open surgical treatment with direct arterial repair and percutaneous/endovascular treatment.
- Factors that are associated with an increased risk for serious complications after catheter removal are catheter diameter, time since catheter insertion and the puncture site.
Recent Comments