
Case contribution: Dr Radhiana Hassan
Clinical:
- A 30 years old lady
- Para 4, post partum day 12
- Presented with yellowish discoloration of skin
- Associated with pale colored stool and tea colored urine
- History of taking multiple medications including herbal supplement for post partum care
- No fever, had mild epigastric pain which was resolved with gastritis medication
- Blood investigation shows feature of obstructive jaundice


Ultrasound findings:
- Liver is homogenous with normal parenchyma echogenicity and echotexture. It has smooth margin.
- Intrahepatic biliary ducts are dilated. Common bile duct is dilated measuring 1.1 cm in diameter.
- There is a hyperechoic focus with posterior shadowing seen within the proximal common bile duct.
- Gallbladder is well distended. Multiple hyperechoic foci with posterior shadowing are detected within the gallbladder the largest measures around 0.9 cm.
- No gallbladder wall thickening or pericholecystic collection.
- Head and body of pancreas are normal.
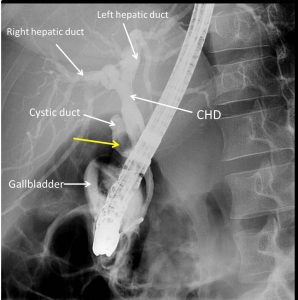
ERCP findings:
- Dilated intrahepatic and common hepatic duct with no filling defect seen within these ducts.
- Filling defect seen within cystic duct (yellow arrow)
- No filling defect in gallbladder
- CBD is not dilated.
- 10fr/8mm stent inserted
- Attempted removal using spiral basket but failed
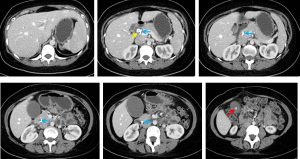
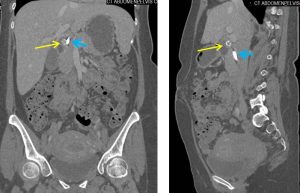
CT scan findings:
- A biliary stent in-situ (blue arrows). Resolution of previously seen dilated intrahepatic ducts and common hepatic duct.
- A calculus measuring about 1.2 cm x1.1 cm x 1.1 cm (AP x W x CC) is noted abutting the lateral aspect of the proximal biliary stent (yellow arrows). This calculus most likely resides within the distal cystic duct causing extrinsic compression towards the CHD rather than residing within the proximal CBD.
- The gallbladder is grossly distended with a calculus seen within, measuring 0.9 cm x 1.0 cm x 1.0 cm (AP x W x CC). No thickening of the gallbladder wall is seen and no pericholecystic fluid is identified.
- The proximal cystic duct is dilated measuring 1.2 cm.
Diagnosis: Mirizzi syndrome type 1
Discussion:
- Mirizzi syndrome is a condition difficult to diagnose and treat
- Diagnostic difficulties are explained by the different clinical presentations of the disease.
- The classic presentation is obstructive jaundice without painful symptoms.
- Ultrasound shows a gallstone impacted in the gallbladder infundibulum causing an external obstruction of the CHD with consequent dilation of the intrahepatic biliary tree. The diagnosis needs to be confirmed by CT or MRI and, finally, by surgery with histological examination.
- Another frequent clinical picture of the Mirizzi syndrome is that of a stricture mimicking biliary cancer. When the associated inflammatory process is predominant, it involves the CBD and mimics a neoplastic stricture at the MR-cholangiography
- A classification system for Mirizzi syndrome is developed based on the degree of bile duct
- Type I: extrinsic compression of the CHD by impacted gallstone in the gallbladder neck or cystic duct
- Type II: erosion of the CHD wall and formation of cholecystocholedochal fistula. The fistula involves less than one third of the circumferential of the CBD.
- Type III: Involvement between one-third and two-third of the circumferential of the CBD
- Type IV: Destruction of the entire wall of the CBD
- Type V: cholecystoenteric fistula together with any other type mentioned above
Progress of patient:
- Elective open cholecystectomy and CBD exploration done
- HPE: chronic cholecytitis
Recent Comments