
Case contribution: Dr Radhiana Hassan
Clinical:
- A 35 years old man with no known medical illness
- Complaint of right temporal swelling and headache
- Initially pain is mild, currently affect his sleep and partially relieved with analgesic
- No fever, no URTI sx. History of MVA a few years ago, no head injury
- Clinically a small swelling at right temporal, firm in consistency. Overlying skin was not inflamed.
- Also had weakness of right facial nerve (temporal part)
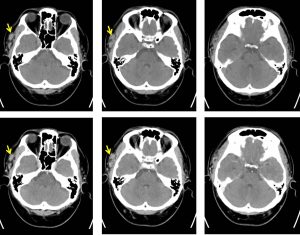
CT scan findings:
- There is heterogeneous lesion seen at the right temporal fossa (yellow arrows) lateral to the right temporalis muscle (HU range 50-60) measuring about 2.5 x 1.1 x 1.1 cm (AP x W x CC).
- Multiple tubular structure with some is slightly prominent seen traversing and supplying the lesion.
- Few fat locules seen entrapped between the lesions.
- No appreciable contrast enhancement is observed in post contrast study.
- The overlying skin and subcutaneous tissue are normal.
- The adjacent bone is not eroded.
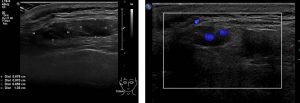
Ultrasound findings:
- There is serpiginous tubular structures with minimal doppler flow at subcutaneous tissue of the right periauricular region. Non-specific waveform patterns are noted.
- It cumulatively measures about 0.7 x 3.2 x 2.0 cm (AP x W x CC).
- No extension to the underlying muscle is noted.
- Ultrasound features are suggestive of vascular lesion likely to represent hemangioma.
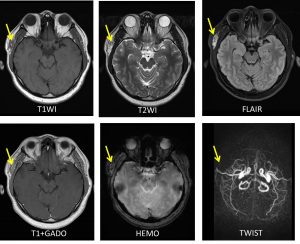
MRI findings:
- There is a superficial, ovoid lesion with a lobulated margin located immediately lateral to the right temporalis muscle.
- The lesion is measuring approximately 2.7 x 0.7 x 2.4 cm (AP x W x CC).
- The lesion appears isointense on T1 and mixed iso and hyperintense on T2-weighted images.
- Heterogenous enhancement is seen post gadolinium.
- Blooming artifacts are seen on HEMO likely due to due to the presence of blood products (no calcification seen in the recent CT).
- No restricted diffusion on ADC/DWI.
- The right frontal branch of superficial temporal artery (branches from right ECA) is seen traversing and insinuating into the lesion. The right scalp vein also appears prominent. However no nidus is identified.
- No dilated tortuous vessel seen or abnormal dilatation of cerebral vein.
- No extension into the orbital or intracranial region.
Progress of patient:
- Excision biopsy of right temporal mass done under GA
- Intraoperative findings show a small cystic lesion about 2×2 cm with blood and serous content just above the temporalis muscle. Excised as whole.
- A review after one year, patient is well with no more headache.
HPE findings:
- Macroscopy: specimen labeled as right temporal cyst consist of a piece of greyish tissue measuring 24x18x5 mm. The cyst is not intact. No content.
- Microscopy: section shows admixture of vascular channels of varying sizes displaying thin and thick muscular wall lined by endothelial cells. Some of the vessels are dilated. The surrounding adipose stroma is hemorrhagic with fibrin. No atypical cells noted. Adjacent skeletal muscles are noted. No evidence of dysplasia or malignancy.
- Interpretation: consistent with arteriovenous malformation.
Diagnosis: Scalp arteriovenous malformations (AVM)
Discussion:
- Scalp AVMs are relatively rare. These lesions may be congenital or may develop after trauma
- They are usually seen during childhood, adolescence, and early adulthood
- MRI can help to distinguish scalp AVMs which are high flow lesions from other low flow lesions such as venous or lymphatic malformations, and this will help with the treatment planning.
- Catheter angiography is still the gold standard modality to understand the angioarchitecture of the lesion and to exclude any intracranial component
- However, in our case the typical imaging features of AVMs are not demonstrated, thus diagnosis of hemangioma was given.
- Thus, I would like to emphasize that mass lesions in the scalp should not be operated on without preoperative meticulous evaluation.
- Scalp AVMs may be treated safely and effectively with a surgical approach following a detailed preoperative evaluation. Surgical excision is the most common and successful method of treating scalps AVMs. Endovascular approaches are an option as a definitive therapy or as an adjunct to surgical therapy to reduce blood loss during excision.
Recent Comments